moralizing
noun
1. A moral reflection; a moralization. Also spelled moralising.
2. The behaviour of one who moralizes.
3. indulgence in moral pronouncements; the exposition (often superficially) of a particular moral code
I profess a Christian belief system and the Good Book has the following text: The heart is deceitful above all things and desperately wicked; who can know it? (Jeremiah 17:9)
While I sense I have experienced some character change, I personally must assume my heart is deceitful and I do not know much of it. So I cannot insist I am not doing as you assert. I also cannot insist that I am. I haven't a clue.
@larry806q wrote: The weirdo kind that cares about their fellow human beings. Those kinds of weirdos.
I honestly believe the covid nightmare may be the most horrible thing ever foisted on this planet and millions will likely die due to the jab so I do know one motive I have. It is an intense concern for humanity.
I continue to see that you made unfounded critical assertions.
And here you add to that. (Grow up and I do not think or talk like an adult.)
You can attempt to justify that allegation, but don't bother on my account.
^
I hate injustice and I am actually much more passionate about responding to perceived injustice when it is done to someone other than myself. (I don't know why this is.)
I thought your first post I responded to was unjust to whomever it was pointed at. I certainly did not take it as pointed at me individually though I certainly saw it as highly probable that I was one of the folks you intended it for.
I responded to your post directed toward me because I think it is totally asinine, unjust, and was directed to me.
I personally do not have an axe to grind with those who don't get vaccinated or don't wear masks in confined public areas. Many of those who don't get vaccinated have legitimate health concerns, and the ones who can't be bothered or believe it is not necessary, well what am I gonna do? I try not to appear to scowl from behind my mask. But I have a real issue with people who push a narrative that the vaccines are more harmful than other vaccines that are used and have been used, Especially given the lethallity of the current pandemic.
I accept that the media is perverted. Any casual observer of the media can see that it is largely a for-profit-business and ripe for manipulation for any number of reasons. I do not think that the news industry should be a for-profit operation.
I also have little respect for the pharmacology industry, another endeavor that is warped by making money. We as a society have been coerced into believing without a doubt that only a profit driven market based economy can keep us from deprivation.
That said, it is clear that the covid-19 pandemic is real, it kills on a massive world wide scale and our struggle to contain it has resulted in economic loss across most of society, myself included.
Those who can't see this are either paranoids, suckers or the willfully obstinate. But the real criminals in this are those in the political elites who have decided it is in their interest to knowingly set common sense aside and stoke the flames of the anti vaxx movement.
I personally do not have an axe to grind with those who don't get vaccinated or don't wear masks in confined public areas. Many of those who don't get vaccinated have legitimate health concerns, and the ones who can't be bothered or believe it is not necessary, well what am I gonna do? I try not to appear to scowl from behind my mask. But I have a real issue with people who push a narrative that the vaccines are more harmful than other vaccines that are used and have been used, Especially given the lethallity of the current pandemic.
I accept that the media is perverted. Any casual observer of the media can see that it is largely a for-profit-business and ripe for manipulation for any number of reasons. I do not think that the news industry should be a for-profit operation.
I also have little respect for the pharmacology industry, another endeavor that is warped by making money. We as a society have been coerced into believing without a doubt that only a profit driven market based economy can keep us from deprivation.
That said, it is clear that the covid-19 pandemic is real, it kills on a massive world wide scale and our struggle to contain it has resulted in economic loss across most of society, myself included.
Those who can't see this are either paranoids, suckers or the willfully obstinate. But the real criminals in this are those in the political elites who have decided it is in their interest to knowingly set common sense aside and stoke the flames of the anti vaxx movement.
I am with you on about 96% of that. Yes it clearly can and does kill (sadly). Without trying to get yet another pissing contest going truly, Cuomo and Whitmer didn't do anyone any favors. There are reports/videos available from Doctors who specialize in respiratory disease that are saying keeping folks laying down and still is counter productive. That known and established remedies such as hydrochloriquine were both removed from treatment and "bad mouthed" didn't save any lives either. That both the college and professional football seasons see full stadiums and zero spikes suggests there may be a fly in the ointment.
I might suggest the media is more in the tank than even you are suggesting. And if you look up evil in the dictionary there is a picture of big pharma. And I can't imagine we are going to argue that politicians are pure of heart for our well fair. Where I do take my 4% is labeling anti-jabbers in a negative manner. If you are right and the vaccine does protect you why does it matter if I am not vaccinated? A case could be made that actually helps you because at some point in time I die, among other things posing no further infection risk. Have you actually taken ANY time to contemplate if I am correct and you are wrong what that portends?
I agree that the economic impact is hideous, truly hideous. I would not agree that it was an attempt to control the virus that is 99.7%+ survivable.
Take a couple of minutes and look up either Davos or the World Economic Forum, those organizations really exist, they aren't someone's opinion.
the thing about viruses is that the are communicable. its the rate of trasmission that is dangerous, covid is upwards of 1:3 where each person shedding the virus can infect 3 people. (Vaccinated people are less likely to become infected with a viral load that is that contagious). And then there is the problem of hospitals being overwhelmed with acutely ill covid patients. That happens, and when it does people die because covid patients need specialized care...more attention. All this has been written about and reported extensively but many many people willfully ignore these reports. In my city I have personally heard accounts from doctors and nurses in hospital who lost patients that would otherwise have lived had they not been so busy with other desperately sick people.
For adults with COVID-19 and shock, the Panel recommends using dynamic parameters, skin temperature, capillary refilling time, and/or lactate levels over static parameters to assess fluid responsiveness (BIIa).
For the acute resuscitation of adults with COVID-19 and shock, the Panel recommends using buffered/balanced crystalloids over unbalanced crystalloids (BIIa).
For the acute resuscitation of adults with COVID-19 and shock, the Panel recommends against the initial use of albumin for resuscitation (BI).
For adults with COVID-19 and shock, the Panel recommends norepinephrine as the first-choice vasopressor (AI).
For adults with COVID-19 and shock, the Panel recommends titrating vasoactive agents to target a mean arterial pressure (MAP) of 60 to 65 mm Hg over higher MAP targets (BI).
The Panel recommends against using hydroxyethyl starches for intravascular volume replacement in patients with sepsis or septic shock (AI).
When norepinephrine is available, the Panel recommends against using dopamine for patients with COVID-19 and shock (AI).
As a second line vasopressor, the Panel recommends adding either vasopressin (up to 0.03 units/min) (BIIa) or epinephrine (BIIb) to norepinephrine to raise MAP to target or adding vasopressin (up to 0.03 units/min) (BIIa) to decrease norepinephrine dosage.
The Panel recommends against using low-dose dopamine for renal protection (AI).
The Panel recommends using dobutamine in patients who show evidence of cardiac dysfunction and persistent hypoperfusion despite adequate fluid loading and the use of vasopressor agents (BIII).
The Panel recommends that all patients who require vasopressors have an arterial catheter placed as soon as practical, if resources are available (BIII).
For adults with refractory septic shock who have completed a course of corticosteroids to treat their COVID-19, the Panel recommends using low-dose corticosteroid therapy (“shock-reversal”) over no corticosteroid therapy (BIIa).
Oxygenation and Ventilation
For adults with COVID-19 and acute hypoxemic respiratory failure despite conventional oxygen therapy, the Panel recommends high-flow nasal cannula (HFNC) oxygen over noninvasive positive pressure ventilation (NIPPV) (BIIa).
In the absence of an indication for endotracheal intubation, the Panel recommends a closely monitored trial of NIPPV for adults with COVID-19 and acute hypoxemic respiratory failure and for whom HFNC is not available (BIIa).
For patients with persistent hypoxemia despite increasing supplemental oxygen requirements in whom endotracheal intubation is not otherwise indicated, the Panel recommends considering a trial of awake prone positioning to improve oxygenation (CIIa).
The Panel recommends against using awake prone positioning as a rescue therapy for refractory hypoxemia to avoid intubation in patients who otherwise meet the indications for intubation and mechanical ventilation (AIII).
If intubation becomes necessary, the procedure should be performed by an experienced practitioner in a controlled setting due to the enhanced risk of exposing health care practitioners to SARS-CoV-2 during intubation (AIII).
For mechanically ventilated adults with COVID-19 and acute respiratory distress syndrome (ARDS):
The Panel recommends using low tidal volume (VT) ventilation (VT 4–8 mL/kg of predicted body weight) over higher VT ventilation (VT >8 mL/kg) (AI).
The Panel recommends targeting plateau pressures of <30 cm H2O (AIIa).
The Panel recommends using a conservative fluid strategy over a liberal fluid strategy (BIIa).
The Panel recommends against the routine use of inhaled nitric oxide (AIIa).
For mechanically ventilated adults with COVID-19 and moderate-to-severe ARDS:
The Panel recommends using a higher positive end-expiratory pressure (PEEP) strategy over a lower PEEP strategy (BIIa).
For mechanically ventilated adults with COVID-19 and refractory hypoxemia despite optimized ventilation, the Panel recommends prone ventilation for 12 to 16 hours per day over no prone ventilation (BIIa).
The Panel recommends using, as needed, intermittent boluses of neuromuscular blocking agents (NMBA) or continuous NMBA infusion to facilitate protective lung ventilation (BIIa).
In the event of persistent patient-ventilator dyssynchrony, or in cases where a patient requires ongoing deep sedation, prone ventilation, or persistently high plateau pressures, the Panel recommends using a continuous NMBA infusion for up to 48 hours as long as patient anxiety and pain can be adequately monitored and controlled (BIII).
For mechanically ventilated adults with COVID-19, severe ARDS, and hypoxemia despite optimized ventilation and other rescue strategies:
The Panel recommends using recruitment maneuvers rather than not using recruitment maneuvers (CIIa).
If recruitment maneuvers are used, the Panel recommends against using staircase (incremental PEEP) recruitment maneuvers (AIIa).
For critically ill patients with COVID-19 who have acute kidney injury and who develop indications for renal replacement therapy, the Panel recommends continuous renal replacement therapy (CRRT), if available (BIII).
If CRRT is not available or not possible due to limited resources, the Panel recommends prolonged intermittent renal replacement therapy rather than intermittent hemodialysis (BIII).
Pharmacologic Interventions
In patients with COVID-19 and severe or critical illness, there is insufficient evidence for the Panel to recommend either for or against empiric broad-spectrum antimicrobial therapy in the absence of another indication.
If antimicrobials are initiated, the Panel recommends that their use should be reassessed daily to minimize the adverse consequences of unnecessary antimicrobial therapy (AIII).
Extracorporeal Membrane Oxygenation
There is insufficient evidence for the Panel to recommend either for or against the use of extracorporeal membrane oxygenation for patients with COVID-19 and refractory hypoxemia
Abstract
SARS-CoV-2, the causative agent of coronavirus disease 2019 (COVID-19), is responsible for the largest pandemic facing humanity since the Spanish flu pandemic in the early twentieth century. Since there is no specific antiviral treatment, optimized support is the most relevant factor in the patient's prognosis. In the hospital setting, the identification of high-risk patients for clinical deterioration is essential to ensure access to intensive treatment of severe conditions in a timely manner. The initial management of hypoxemia includes conventional oxygen therapy, high-flow nasal canula oxygen, and non-invasive ventilation. For patients requiring invasive mechanical ventilation, lung-protective ventilation with low tidal volumes and plateau pressure is recommended. Cardiovascular complications are frequent and include myocardial injury, thrombotic events, myocarditis, and cardiogenic shock. Acute renal failure is a common complication and is a marker of poor prognosis, with significant impact in costs and resources allocation. Regarding promising therapies for COVID-19, the most promising drugs until now are remdesivir and corticosteroids although further studies may be needed to confirm their effectiveness. Other therapies such as, tocilizumab, anakinra, other anti-cytokine drugs, and heparin are being tested in clinical trials. Thousands of physicians are living a scenario that none of us have ever seen: demand for hospital exceed capacity in most countries. Until now, the certainty we have is that we should try to decrease the number of infected patients and that an optimized critical care support is the best strategy to improve patient’s survival.
Introduction
Since December 31, 2019, when China reported a series of cases of acute respiratory failure caused by a new species of coronavirus, SARS-CoV-2, more than 50 million new cases and almost 1,260,000 deaths have been confirmed worldwide. In Brazil, 5,664,115 cases were reported with 162,397 deaths from the disease by November 8th, 2020 [1]. Its rapid spread and high lethality, especially in the most fragile groups such as the elderly and those with comorbidities, make this pandemic a new challenge faced by modern medicine.
The pathophysiology of COVID-19 is complex, and the disease may compromise lung, heart, brain, liver, kidney, and of the coagulation system. COVID-19 can result in myocarditis, cardiomyopathy, ventricular arrhythmias, acute coronary syndrome, and shock [2,3,4,5,6,7,8]. Venous and arterial thromboembolic events occur in 31–59% of hospitalized patients with COVID-19 [5, 6].
This publication aims to provide a specialist consensus on specific management of COVID-19 in intensive care, covering from the admission criteria in the intensive care units (ICU) to antiviral treatment, with sections on ventilatory, hemodynamic, and metabolic support. We searched PubMed, Medrxiv, and Embase using the search terms coronavirus, COVID-19, SARS-CoV-2, severe acute respiratory syndrome COVID-19, critically ill, and intensive care unit for studies published from December 31, 2019, to June 11st, 2020, and selected manually the relevant articles. We selected articles relevant to a general medicine readership, prioritizing randomized clinical trials, systematic reviews, and clinical practice guidelines.
ICU admission criteria for adult patients infected with COVID-19
Authorities from the Chinese Center for Disease Control and Prevention reported that, among more than 44,000 confirmed cases of COVID-19, about 81% were asymptomatic or presented mild symptoms such as cough, fever, fatigue, and myalgia [9]. Although for these cases, home management and self-isolation are the appropriate measures, 14% developed a severe form of the disease and 5% were critical, requiring hospitalization and ICU admission, respectively [9]. Severe patients with COVID-19 usually present respiratory rates ≥ 30 breaths per minute, oxygen saturation ≤ 93%, and lung infiltrates > 50% [9], and are at high risk for clinical deterioration and for developing critical illness, including acute respiratory distress syndrome (ARDS) [10]. Hospitalization should be warranted for patients who develop severe symptoms; however, ICU admission has been reserved for the most severe forms, depending on the capacity of the health care system. Despite differences in culture and practices around the world, most centers report that around 25% of hospitalized patients require ICU admission [11, 12].
Patients with the severe form of the disease must be closely monitored, since rapidly progression from moderate to severe ARDS may occur. Acute hypoxemic respiratory failure is the most common complication occurring in 60–70% of patients admitted to the ICU [11]. Patients at high risk for ARDS development are those older than 65 years old, presenting high fever (T > 39ºC), neutrophilia, lymphocytopenia, elevated markers of hepatic and renal failure (aspartate aminotransferase, alanine aminotransferase, creatinine, and urea), elevated acute-phase proteins as markers of inflammation (high-sensitivity C-reactive protein, procalcitonin, and serum ferritin), and elevated coagulation function-related indicators (prothrombin time, fibrinogen, and D-dimer) [1, 10].
Admission criteria include oxygen requirements equal or superior to 6–8 l/min to reach a peripheral oxygen saturation ≥ 90–92%, respiratory failure, shock, acute organ dysfunction, and patients at high risk for clinical deterioration. However, in many countries, due to the shortage of ICU beds, usually only patients requiring intubation and invasive mechanical ventilation were admitted to ICU.
Pulmonary impairment, physiopathology, and ventilation strategies
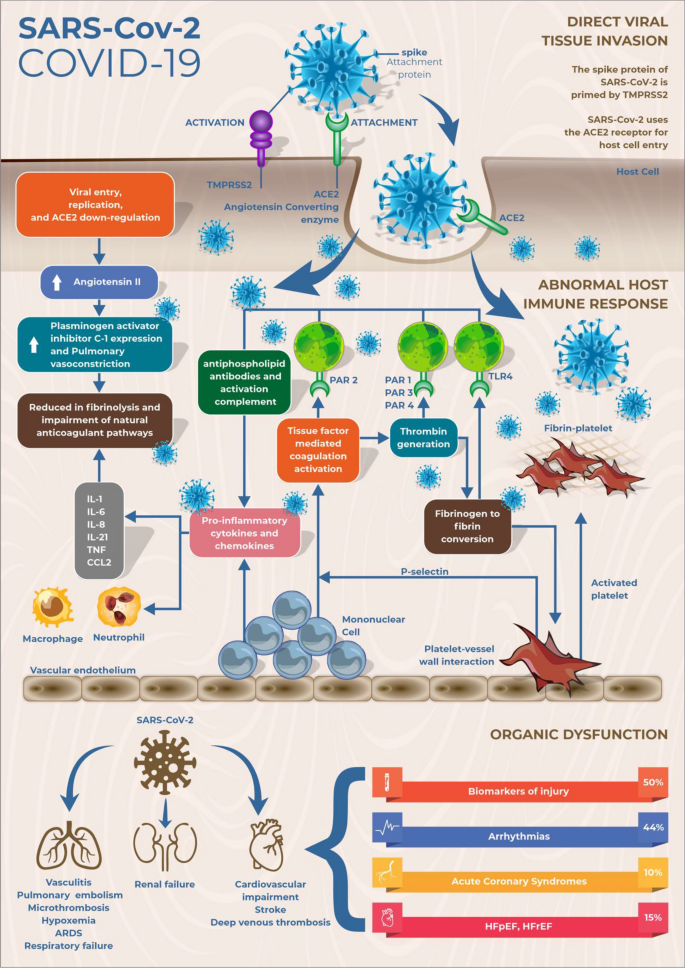
The pathophysiology of COVID-19-induced ARDS involves characteristic properties which make it different from other causes of ARDS: patients present an intense endothelial dysfunction with a thromboinflammatory state. Multiple mechanisms of dysregulation in the pulmonary perfusion exist in COVID-19: the abolition of hypoxic pulmonary vasoconstriction, excessive pulmonary vasoconstriction; and microthrombosis or macrothrombosis, leading to increased dead space [13, 14]. Pulmonary microthrombosis and endothelial damage that result in V/Q (ventilation/perfusion) mismatch, hypoxemia, and vasodilation (Fig. 1) [15,16,17]. Increased inflammatory and thrombotic biomarkers are associated with severe clinical presentation and mortality in COVID-19 patients. High levels of D-dimer, IL-6, C-reactive protein, procalcitonin, troponin, LDH, and ferritin are detected in severely ill patients [18].
Fig. 1
The pathophysiology of SARS-CoV-2 infection. SARS-CoV-2, via its surface spike protein, binds to the human ACE2 receptor after spike protein activation by TMPRSS2. This results in down-regulation of ACE2 and increased angiotensin II levels and consequently increased plasminogen activator inhibitor C-1 expression and reduced fibrinolysis. The disease it causes is associated with an increase in inflammatory cytokines and coagulation disorders, with predisposition to thrombus formation. Mononuclear cells interact with activated platelets and the coagulation cascade, which activate 1 inflammatory cells by binding thrombin and tissue factor with specific protease activated receptors and by binding fibrin to Toll-like receptor 4. The activation of inflammatory cells results in the release of pro-inflammatory cytokines, leading to impairment of the natural coagulation pathways and shut down of fibrinolysis. This state of hyper inflammation and hypercoagulability leads to multiple organ dysfunction, most commonly affecting the lungs, heart and kidneys. ACE2 angiotensin-converting enzyme-2, aPTT activated partial thromboplastin time, ARDS acute respiratory distress syndrome, COVID-19 coronavirus disease 2019, HFpEF heart failure preserved ejection fraction, HFrEF, heart failure reduced ejection fraction, IL interleukin, PAR protease-activated receptor, PT prothrombin time, SARS-COV-2severe acute respiratory syndrome coronavirus 2, TMPRSS2 transmembrane protease serine, TLR4 Toll-like receptor 4, TNFα tumor necrosis factor-α
Full size image
Hospitalization trends vary with age and may reach around 20% of COVID-19 patients [19]. In hospitalized patients, ventilatory support may vary from the need for O2 supplementation through a nasal catheter to invasive mechanical ventilation or extracorporeal membrane oxygenation (venovenous ECMO) in patients with the most severe forms of ARDS. In general, patients must be maintained with the minimum amount of supplemental O2 for a SpO2 between 92 and 96%. Without BGA, the degree of hypoxemia can be estimated by SpO2/FiO2 ratios, with values ≤ 315 suggesting ARDS [20].
Non-invasive ventilation: Health services have been and are predicted to be overloaded in most large centers as a result of the spreading COVID-19 pandemic, leading mainly to the lack of ICU beds and insufficient number of mechanical ventilators for patients who need them [21]. Many hospitals have adopted non-invasive ventilation (NIV) as an attempt to prevent respiratory failure from evolving into severe forms that require invasive ventilatory support.
Both the European Society for Intensive Care Medicine (ESICM) with the international Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with coronavirus disease 2019 (COVID-19), and the National Health Service of England (NHS-England) recommend the use of NIV as an initial measure for respiratory failure in patients with COVID-19 (weak recommendation, low-quality evidence) [22, 23]. It is still an ongoing debate about which would be the most recommended non-invasive interface and technique: NIV devices such as BIPAP, or the use of high-flow nasal cannulas (HFNC).
The prone position in non-intubated patients were tested in some initial studies [24,25,26]. Patients who tolerated more than 3 h in prone position present a substantially improve in oxygenation from supine to prone positioning. However, only about half of the patients maintain the benefit after resupination [25, 26]. Further studies are needed to reinforce the real benefit of this intervention.
Invasive mechanical ventilation
ARDS is defined as a form of inflammatory pulmonary edema of non-cardiogenic etiology, with a reduction in the areas of normoventilated lung and consequent reduction in respiratory compliance and shunt effect. The Berlin definition proposed categories of ARDS based on degree of hypoxemia: mild (200 mmHg < PaO2/FIO2 ≤ 300 mmHg), moderate (100 mmHg < PaO2/FIO2 ≤ 200 mmHg), and severe (PaO2/FIO2 ≤ 100 mmHg) and variables for severe ARDS: radiographic severity, respiratory system compliance (≤ 40 mL/cm H2O), positive end-expiratory pressure (≥ 10 cm H2O), and corrected expired volume per minute (≥ 10 L/min) [27].
To manage these patients, maneuvers that lead to recruitment of collapsed areas are usually applied, such as increased positive end-expiratory pressure (PEEP), alveolar recruitment maneuvers, and prone position, leading to a reduction in elastance and increased compliance [28]. Prone positioning presents the potential benefit of a relieve of severe hypoxemia due to reduction of overinflated lung areas, promoting alveolar recruitment and decreasing ventilation/perfusion mismatch. This intervention might be considered in patients with PO2/FiO2 < 150, in the absence of contraindications [29, 30]. The main objective of mechanical ventilation in these patients is to maintain a lung-protective strategy for all patients with ARDS, defined as targeting a tidal volume of 4 to 8 mL/kg predicted body weight (PBW) and a plateau pressure of less than 30 cmH2O [28].
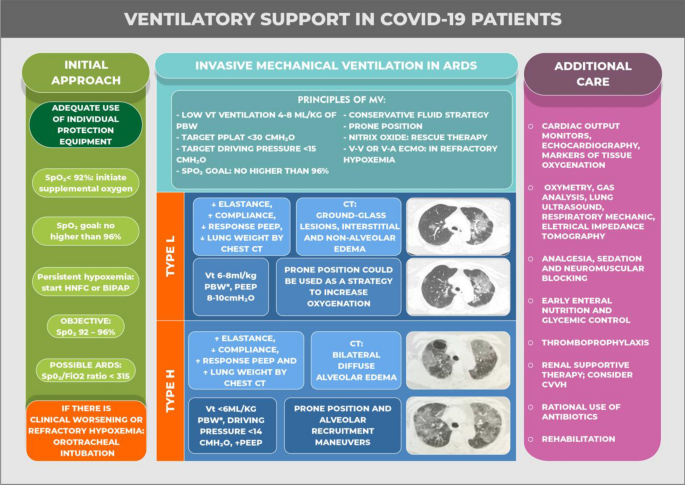
A group of experts hypothesize that in COVID, there may be two phenotypes of ARDS [21]. Patients often exhibit normal compliance even in the presence of severe hypoxemia, with normal or even increased minute ventilation, and more than half of these patients do not appear dyspneic. Radiologically, such patients have ground-glass tomographic lesions indicative of interstitial and non-alveolar edema, and these infiltrates are relatively limited in extent at this stage. These patients are called “type L” (“low elastance”), with additional main characteristics of high compliance, low response to PEEP, and low lung weight estimated by chest computed tomography (CT) [21]. Patients may evolve with progressive clinical improvement or, whether due to individual predisposing factors or inadequate management, evolve with a more severe form closer to the classic ARDS. This is named as “type H” (from “high elastance”), showing also low compliance, high response to PEEP, and high lung weight estimated on chest CT [31]. It should be highlighted that this division is conceptual, to facilitate the understanding of the respiratory condition, with types “H” and “L” representing the ends of a spectrum that frequently overlap [31].
Mechanical ventilation strategy according to patient phenotypes (“type L” or “type H”)
In severe cases of respiratory failure, as frequently seen in SARS-CoV-2-related ARDS, severe hypoxemia can lead to a persistent increase in respiratory effort, with consequent self-induced lung injury (P-SILI). In addition, other factors such as fluid overload or SARS-1 CoV-2-induced myocardial injury may also play important roles in worsening of the condition through pulmonary congestion [32]. Thus, a mechanical ventilation strategy must take into account the multiple mechanisms of lung injury and the different presentations of the disease—conventional form of ventilation in ARDS will not always be the most appropriate, as described below [31].
Type L: it is suggested to ventilate “type L” patients, typically patients with good lung compliance, higher tidal volumes (VT) (around 7–8 mL/kg of ideal body weight). Higher VT helps to avoid reabsorption atelectasis and hypercapnia due to limited VT-induced hypoventilation. The rationale behind this strategy is as follows: the initial feature of these patients is the vasoregulation defect in the pulmonary capillaries—the reflex vasoconstriction that normally occurs in response to hypoxemia is not found in these patients due to endothelial changes and microthrombosis. Elevation of FiO2 may be sufficient in most patients not experiencing excessive respiratory effort, with maintenance of NIV with BIPAP or HFNC leading to slow and progressive improvement of hypoxemia and reversal of ARDS. However, if the inflammatory condition progresses, or if the patient's ventilatory effort is excessive, secondary pulmonary tissue stress may lead to P-SILI, with severe deterioration of lung function. At this point, intubation with adequate sedation/paralysis can interrupt the vicious cycle. These patients should be ventilated with lower PEEP (between 8 and 10 cmH2O) to avoid redirection of blood flow away from the aerated pulmonary capillaries, which would increase the shunt effect. As capillary hypoperfusion can also suffer a gravity-dependent effect, the prone position could be used as a strategy to minimize it and increase oxygenation.
Type H: with disease progression and worsening of inflammatory edema, the patient may progress to “type H”. The pathophysiology of this progression is probably the result of a combination of factors: in addition to self-induced lesion (P-SILI), the viral lesion itself leads to uncontrolled inflammation and edema, with local and generalized thrombogenesis, intense release of cytokines, and right ventricular overload. The resulting pulmonary edema is close to classic ARDS presentation, with collapsed alveoli and extensive normoperfused and hypoaerated areas. In these more advanced cases, a mechanical ventilation strategy should be more traditional: elevated PEEP, VT < 6 mL/kg, driving pressure < 14 cmH2O, prone position, and alveolar recruitment maneuvers in refractory cases.
As previously stated, categorization in two different profiles facilitates clinical management by indicating the need for different ventilatory approaches. However, due to the frequent overlap of the two types, individualization of ventilatory management is essential. In either case, patients with COVID-19 who undergo mechanical ventilation have an average recovery time of 1–3 weeks [33, 34]. The progress toward improvement is characteristically slow; therefore, prolonged sedation is often unavoidable. In most severe cases of ARDS and also in cases of non-protective ventilation or in the occurrence of asynchrony, neuromuscular blockage is useful, and complications such as polyneuropathy of the critically ill patient are usually diagnosed. Figure 2 shows the main principles of the management of COVID-19 respiratory failure.
Full size image Cardiovascular impairment, physiopathology, and treatment strategies
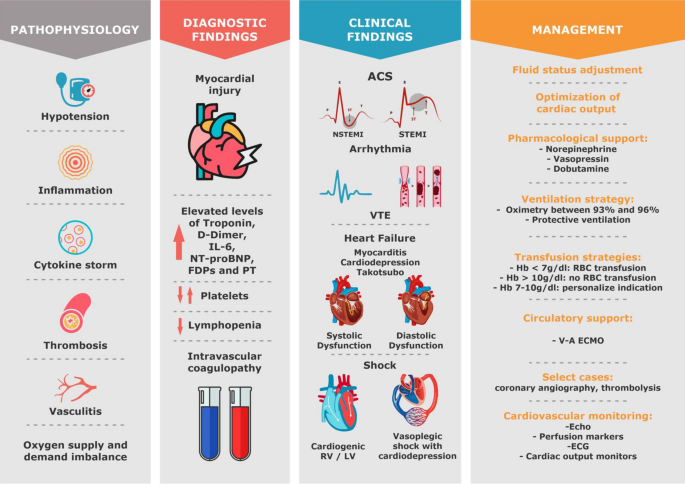
Cardiac injury is a common occurrence in patients with COVID-19. Multiple mechanisms are involved: virus direct toxicity, inflammation, thrombogenesis, endothelial injury, sympathetic overstimulation, myocarditis, hypoxemia, vasoconstriction, supply/demand disorder, low cardiovascular and respiratory reserve, and secondary infections. Different phenotypes result from this: cardiac injury alone, myocarditis with heart failure, arrhythmias, venous and arterial thromboembolism, acute coronary syndrome, and shock (Fig. 3) [4, 35, 36].
Fig. 3
Cardiovascular involvement in patients with COVID-19; pathophysiology, diagnostic findings, most common clinical findings and proposed management. IL-6 interleukine-6, FDPs fibrin degradation product, PT prothrombin time, ACS acute coronary syndrome, NSTEMI non-ST elevation myocardial infarction, STEMI ST elevation myocardial infarction, VTE venous thromboembolism, RV right ventricle, LV left ventricle, Hb hemoglobin, V-A venous-arterial, Echo echocardiography, ECG electrocardiogram
Full size image
A recent study that included 100 patients with COVID-19 submitted to echocardiography within 24 h of admission showed that the most common findings were right-ventricular (RV) dilatation and dysfunction (39% of patients), followed by left-ventricular (LV) diastolic dysfunction (16%) and LV systolic dysfunction (10%) [37]. In hospitalized patients with confirmed COVID-19, the incidence of shock is 20–35% [38, 39]. Among patients 1 who received IMV, about 95% may need vasopressor support [40].
The main goal of shock and hemodynamic instability management of patients with COVID-19 severe illness is to restore arterial pressure and to optimize cardiac output with the ultimate goal to improve or preserve organ perfusion. Severe lung injury and mechanical ventilation also contribute to deleterious hemodynamic effects. The extensive viral infection and ARDS induced by COVID-19 results in diffuse lung inflammation, consolidation, marked microvascular thrombosis, endothelial dysfunction, and vasoconstriction [41]. In addition, hypoxemia and dead space lead to a rise in pulmonary vascular pressure and resistance and right-ventricular (RV) afterload increase [42].
The increase in RV afterload and preload may result in RV dilatation, in a septal shift toward the left ventricle (LV) and then in a decrease in LV filling that eventually result in low cardiac output and hemodynamic deterioration [42].
Acute Cor Pulmonale (ACP) is a relatively common occurrence in severe COVID-19 patients. In some patients, ACP can be the result of acute pulmonary embolism, a frequent event in the course of COVID-19 [43], which should prompt a specific therapy [44].
A conservative fluid strategy is usually recommended in patients with ARDS. Aggressive fluid administration and hypervolemia is associated with longer ICU stay, prolonged ventilator dependence, and higher mortality [22, 42, 45, 46]. However, hypovolemia can occur in COVID-19, especially in the early phase, or even in later phases due to intense associated sepsis (increased capillary leakage and increased venous capacitance). Uncorrected hypovolemia may lead to peripheral organ hypoperfusion, facilitate thrombi formation in the context of severe COVID-19 coagulopathy, and might even aggravate hypoxemia due to a low PvO2 effect in case of high degree of pulmonary shunt fraction. It is thus important to assess the benefit/risk ratio of fluid administration. The expected benefit could be assessed by performance of fluid responsiveness tests, administering bolus of hypotonic crystalloids (lactated`s Ringer), and evaluating dynamic variables such as cardiac index and velocity–time integral [47]. Use of tidal volume challenge assessing the changes in pulse pressure variation during a transient increase in tidal volume (e.g., from 6 to 8 mL/kg) [48] is an excellent option in COVID-19 ARDS patients often deeply sedated. If available, advanced hemodynamic monitoring technologies 1 such as transpulmonary thermodilution may help assessing the fluid infusion benefit/risk ratio.
Additionally, COVID-19 myocardial depression may develop at any phase of the disease, sometimes with fulminant myocarditis which might occur in about 1% of hospitalized patients [49, 50]. Early detection of myocardial involvement through the measurement of troponin and natriuretic peptide concentrations and echocardiography is recommended [4, 11]. A recent paper showed that even in less severe forms of disease, myocardial inflammation may persist in almost 60% of patients 70 days after disease [51]. Point-of-care echocardiography might help in the diagnosis of shock and in the non-invasive assessment of preload responsiveness [47, 52,53,54].
Norepinephrine is the first-line vasopressor in patients with hemodynamic instability and COVID-19 [22, 45, 55]. In patients with ARDS, norepinephrine also can improve RV function by restoring mean arterial pressure and thus RV blood supply [42]. If norepinephrine is unable to achieve adequate mean arterial pressure, vasopressin could be added as a second-line vasoactive agent to reach the target blood pressure [22]. Vasopressin might be used as first vasopressor, mainly in cases of atrial fibrillation, pulmonary hypertension, and acute renal failure [56]. Angiotensin 2 (Ang-2) has also been successfully used in COVID-19 patients in a few cases [57]. Although there are no definite trials to support Ang-2′s superiority over conventional vasopressors in COVID patients with vasodilatory shock, there is a physiologic rationale for using the drug. Dobutamine is the inotropic agent the most used in case of acute heart failure. It is indicated in the presence of cardiac dysfunction and in the occurrence of tissue hypoxia after fluid status adjustment and norepinephrine administration.
Prone positioning and inhaled selective pulmonary vasodilators have been used for patients with refractory hypoxemia; moreover, they may have a beneficial hemodynamic effect in particular by decreasing RV afterload and restoring RV function [58, 59]. Finally, in cases of refractory ARDS combined or not with refractory cardiogenic shock requiring high vasoactive doses, venovenous or veno-arterial ECMO might be considered to restore blood oxygenation and provide hemodynamic stability [60]. Although many new centers have been created and ECMO services are now available worldwide, access to ECMO is restricted, especially in low-income countries. Establishing models of care, in which severely ill patients who are eligible for ECMO are evaluated by systems that can be used to rapidly transfer and group high numbers of critically ill patients would be important to provide high-quality ECMO care during the pandemics. Another issue of interest in ECMO management is that the SARS-CoV-2-induced infection may be associated with higher rates of thrombotic events of the extracorporeal system during V-V ECMO therapy [61].
Renal impairment, physiopathology, and treatment strategies
Although respiratory failure is the main dysfunction caused by SARS-CoV-2, other organs can also be affected, with cardiac and renal failures as the most relevant disorders [62]. Acute kidney injury (AKI) was present in 6.7% with a mortality rate as high as 91.7% in SARS-CoV (causative agent of SARS) [63]. Among 99 ICU COVID-19 patients, Fominsky et al. found that 72 (75.0%) developed AKI and 17 (17.7%) received continuous renal replacement therapy (CRRT) [64].
In a prospective cohort study that included 701 patients diagnosed with COVID-19, the assessment of renal function at admission showed that serum creatinine was elevated in 14.4% and urea in 13.1% of patients [65]. Abnormalities in the coagulation pathway, including prolonged partial thromboplastin time and high D-dimer, were more common in patients with elevated baseline serum creatinine. The risk factors associated with mortality were: proteinuria in any degree, hematuria, elevated basal creatinine, and renal failure AKIN (Acute Kidney Injury Net) 2 or more. There was a correlation between severity of kidney injury (AKIN stages) and death, with a fourfold higher risk of mortality among those with stage 3 AKIN [65].
COVID-19 nephropathy
Findings like proteinuria and hematuria can occur after COVID-19 infection, with some individuals showing signs and symptoms of AKI. It has been demonstrated that RNA viruses are present in urine and renal tissue, indicating that the kidney may also be a target of COVID-19 infection 1 through direct viral invasion in the tubules and renal interstitium [66, 67].
Renal histopathology was examined in a series of autopsies of 26 patients who died of respiratory failure secondary to COVID-19. All patients had evidence of acute tubular injury of varying severity, and a number of other histopathological findings including clusters of erythrocytes and hemosiderin pigments were also present. Of the nine samples tested for the intracellular virus, coronavirus-like particles were identified in seven [66].
Renal failure due to COVID-19 has a multifactorial etiology, with three main mechanisms involved: cytokine injury, organ crosstalk, and systemic effects of infection [68].
Cytokine injury
Cytokine storm through release of IL-6/JAK2/STAT3/SOCS3 and NF-κB (p65)/IL-18 could work together to induce AKI and increase overall renal-related diagnostic markers [69]. McElvaney OJ et al. showed that IL-1β, IL-6, IL-8, and sTNFR1 were all increased in patients with COVID-19. COVID ICU patients could be clearly differentiated from COVID stable patients, and demonstrated higher levels of IL-1β, IL-6, and sTNFR1 [70]. The contribution of increased vascular permeability and volume depletion, as well as cardiomyopathy—which can lead to type I cardiorenal syndrome—in addition to cytokine activation, is yet to be established. Removing cytokines with extracorporeal therapies, often studied as a promising approach in patients with sepsis and AKI, has been proposed in patients with COVID-19 who develop acute renal failure [7, 71].
Organ crosstalk
Connection between alveolar injury and tubular injury has been proven. A retrospective study that included 357 patients with ARDS without kidney disease or AKI at presentation reported that 68% of patients developed AKI. Positive fluid balance, greater disease severity, older patients, and diabetes were independently associated with the development of AKI [72].
Systemic effects
Hemodynamic instability associated with rhabdomyolysis, metabolic acidosis, and hyperkalemia can also occur in COVID-19 patients and contribute to AKI.
Treatment
The indications for renal replacement therapy (RRT) for AKI in critically ill patients are well stablished, regardless of patients' COVID-19 status. However, in an intensive care services overload scenario, providing RRT to an increasing number of patients may exceed the capacity 1 of available machines, supplies, and specialized staff.
In patients without indication of RRT, conservative treatment includes: appropriate dose-loop diuretics (oral or intravenous) for fluid overload and active management of hyperkalemia and metabolic acidosis with potassium binders and sodium bicarbonate. For patients that do not respond to conservative treatment, RRT is indicated.
The use of CRRT remains preferred among critically ill patients with AKI. Even among hemodynamically stable patients who can tolerate intermittent hemodialysis, CRRT, or sustained low-efficiency dialysis (SLED) are preferred, depending on machinery and staff availability and expertise. CRRT or SLED can be managed without 1:1 nursing support, which could potentially help in minimizing the waste of personal protective equipment and limit exposure among nurses on hemodialysis [73].
Regional citrate is the most used anticoagulation strategy during hemofiltration or dialysis. However, some case reports suggest that circuit thrombosis during RRT occurs more frequently in patients with COVID-19 than in other patients, and in these cases, the addition of therapeutic anticoagulation with non-fractioned heparin might be considered [74].
Metabolic impairment and treatment strategies
Data suggest that diabetes, hypertension, and cardiovascular diseases (CVD) are the most common comorbidities related to COVID-19, although prevalence rates vary among different studies. In a pooled data from 10 Chinese studies, prevalence of hypertension, diabetes, and CVD was 21, 11, and 7%, respectively [75].
Recent data suggest that diabetic patients with COVID-19 are more often associated with most severe forms of the disease, varying between 14 and 32% in different studies, with an odds ratio of 2.34 for ARDS compared with patients without diabetes [10].
A study from Wuhan with 161 patients with COVID-19 demonstrated a delayed viral clearance in patients with diabetes. It has been proposed that, in addition to the usual mechanisms (impaired neutrophil chemotaxis, and phagocytosis) by which diabetes predisposes to infections 1 in general, other specific factors related to SARS-CoV-2 can have roles in the increased risk and severity of the disease in diabetes, as following [76]:
Increased expression of angiotensin-converting enzyme-2 (ACE2): acute-phase hyperglycemia results in increased ACE2 expression, which can facilitate the entry of viral cells; however, chronic hyperglycemia reduces expression of ACE2, leading to an increased vulnerability to the inflammatory and harmful effects of the virus [77]. In addition, in pancreatic islets, the effect of SARS-CoV on ACE2 blood glucose receptors can lead to hyperglycemia, even in patients without pre-existing diabetes. In patients with SARS-CoV hyperglycemia persisted for up to 3 years after recovery, indicating transient damage to beta cells [78].
Increased furin: the amount of furin, a membrane-linked protease belonging to the subtilisin/cexinfamily proprotein convertase (PCSK), increases in diabetic individuals. Its role in entry of viruses into the cell, acting as a facilitator for viral replication, has been demonstrated [79].
Impaired T-cell function: lymphocytopenia was observed in patients with COVID-19 and was correlated with a worse prognosis [80].
Increased interleukin-6 (IL-6): IL-6 levels are higher in patients with diabetes. Moreover, it is one of the most relevant cytokines activated in cytokine storm in COVID-19 patients. Thus, it may play a more deleterious role in SARS-CoV-2 infection.
Another potential pathway that may explain the correlation between COVID-19 and diabetes involves the enzyme dipeptidyl peptidase-4 (DPP-4), one of the main targets of pharmacological treatment in patients with type 2 diabetes. DPP-4 works as a functional receptor for MERS-CoV in vitro. Despite direct participation of DPP-4 in glucose and insulin metabolism in type 2 diabetes, it has been shown to also increase inflammation. However, a possible role in SARS-CoV-2 infection and whether treatment of diabetes with DPP-4 inhibitors could alter the course of COVID-19 infection are not known yet [81].
Glycemic control
Monitoring blood glucose levels is an important factor in acute stage and follow-up, especially in those receiving corticosteroid therapy. To date, limited data are available on the association of blood 1 glucose levels and COVID-19; however, data from SARS and H1N1 infections have shown that poor glycemic control increases the risk of complications and death [82].
Thereby, the recommendations for critically ill patients with COVID-19 are:
Monitor blood glucose in infected patients;
Glycemic control in patients already known to be diabetic: collection of plasma glucose, electrolytes, and pH;
Liberal indication for early use of intravenous insulin in severe cases (ARDS and shock), avoiding subcutaneous use;
Therapeutic objectives:
Blood glucose between 72 and 144 mg/dL or 4–16 mmol/L;
In elderly patients (> 70 years) or fragile: blood glucose minimum 90 mg/dL or 5 mmol/L [83].
Specific treatment
Several drugs have been studied for the treatment of the SARS-CoV-2. Most studied antivirals in this scenario were the combination of lopinavir–ritonavir and remdesivir [84, 85]. Currently, the antiviral therapy that appears most promising is remdesivir. This is a prodrug of a nucleotide analogue that is intracellularly metabolized to an analogue of adenosine triphosphate that inhibits viral RNA polymerases. In previous studies, remdesivir was shown to have in vitro activity against Ebola and several coronaviruses, showing a prophylactic and therapeutic efficacy in nonclinical models [86, 87].
Remdesivir has been used recently on a compassionate basis, due to a lack of proven efficacy drugs. A multicenter RCT including 1063 patients receiving remdesivir or placebo showed that remdesivir use led to a significantly shorter duration of hospital stay (11 vs. 15 days), and lower mortality (8% vs. 11.6%) [88]. The FDA has approved this drug for urgent use in COVID-19, it is prescribed intravenously (200 mg IV day 1, and 100 mg IV from day 2 to day 10). A paper published by the same group of authors showed that 5 days of therapy were as effective as 10 days [89].
The antivirals lopinavir/ritonavir, ribavirin, atazanavir, and favipiravir are being tested in the context of COVID-19. Previous in vitro studies suggested that lopinavir presents inhibitory activity against SARS-CoV and MERS-CoV [90,91,92]. Cao B et al. demonstrated in an RCT with 199 hospitalized patients with respiratory failure that lopinavir/ritonavir did not result in any clinical benefit beyond standard care [84]. A recent multicenter trial tested the combination of lopinavir/ritonavir with interferon beta-1b and ribavirin, and confirmed that in comparison with standard care, the combination of drugs resulted in shorter duration of viral shedding and hospital stay and in clinical improvement [93].
As adjuvant therapies in the treatment of COVID-19, chloroquine and hydroxychloroquine have been evaluated in experimental and clinical studies. These drugs have the ability to increase the endosomal pH of cells and reduce replication of SARS-CoV-2 in vitro [94, 95]. However, initial clinical studies have not revealed any clinical benefit for using these drugs either alone or in combination with azithromycin [96, 97]. Cavalcanti et al. in a randomized clinical trial with 667 hospitalized patients with suspected or confirmed COVID-19 who presented with mild-to-moderate manifestation, the use of hydroxychloroquine, alone or with azithromycin, did not improve clinical status at 15 days as compared with standard care [98]. Similarly, the use of hydroxychloroquine has not been beneficial in preventing the development of COVID-19 in patients after high-risk exposure [99]. The routine use of these drugs is not recommended.
In addition, Mercuro et al., in a cohort of 90 patients, showed that hydroxychloroquine in COVID-19 patients was associated with a high risk of QTc prolongation, and concurrent treatment with azithromycin resulted in greater changes in QTc. We recommend that physicians carefully evaluate the benefits and potential risks of this drug [100].
The use of corticosteroids reduces mortality in COVID-19 patients needing respiratory support [101]. The trial showed that dexamethasone 6 mg once a day for 10 days results in lower 28-day mortality among those who were receiving either invasive mechanical ventilation or oxygen. Usual regimens of steroids usually prescribed in ARDS which might be considered in COVID-19 include intravenous methylprednisolone 0.5 mg/Kg twice a day for 5 days, dexamethasone 6 mg once a day for 10 days or dexamethasone 20 mg once a day for 5 days followed by dexamethasone 10 mg once a day for 5 days [102,103,104]. A recent meta-analysis included 678 patients who received steroids during COVID-19 (hydrocortisone, dexamethasone, or methylprednisolone) and showed that the administration of systemic corticosteroids, compared with usual care or placebo, was associated with lower 28-day all-cause mortality [105].
Immunomodulatory drugs such as tocilizumab (antihuman IL-6 receptor antibody), sarilumab (anti-IL6 receptor), anakinra (anti-IL1), reparixin (anti-IL8), interferon-α, and complement inhibitors have been explored as potential therapeutic drugs to improve outcomes in COVID-19 patients [106,107,108,109,110].
Tocilizumab use has been associated with reduced mechanical ventilation and reduced serum IL-6 in these patients [109, 110]. The benefit may be related to the phenotype of intense inflammation, characterized by high levels of IL-6, D-dimer, C-reactive protein, LDH, and ferritin. Its preferential use must be carried out through clinical research protocols [111]; patients admitted early to the ICU and still not intubated are probably who mostly benefit. Two retrospective studies showed efficacy of tocilizumab in COVID-19 [112, 113]. However, 4 randomized studies did not confirm the efficacy of tocilizumab in COVID-19 [114,115,116,117].
Convalescent plasma has been used for the treatment of infectious diseases since the early twentieth century with reduced mortality in cases series and case reports during the 1918 influenza, the 2003 SARS, and the 2009 influenza H1N13 pandemics [118]. In COVID-19, several uncontrolled case series of convalescent plasma use were performed, suggesting a survival benefit [119, 120].
Li et al. published the first RCT of convalescent plasma in COVID-19, showing no significant benefit in clinical improvement or mortality. However, this study suggests possible benefit in the subgroup of severely ill patients. Further clinical trials are needed to establish the clinical indications for antibody therapies against COVID-19 [98].
Antithrombotic treatment
Progressive respiratory failure is the primary cause of death in the COVID-19 pandemic, followed by cardiovascular complications. Pathological studies performed in COVID-19 patients showed severe endothelial injury, associated with the presence of intracellular virus and disrupted cell membranes. Pulmonary vessels had widespread thrombosis with microangiopathy and alveolar microthrombi [121]. A Brazilian study of 10 minimally invasive autopsies revealed the presence of diffuse alveolar damage in the lung, and epithelial viral cytopathic effects in alveolar and small airway epithelia. A variable number of small fibrinous thrombi in small pulmonary arterioles were found in areas of both damaged and preserved lungs. Signs of bacterial pneumonia were observed in 6 of 10 cases [122].
In patients who died from COVID-19-associated or influenza-associated respiratory failure, the histologic pattern in the peripheral lung was diffuse alveolar damage with T-cell infiltration. However, increased thrombogenesis was 9 times more prevalent in patients with COVID-19 than in influenza patients [121]. COVID-19 has been described as a thromboinflammatory disease [15] with thrombogenesis a consequence of severe endothelial injury, exacerbated inflammation, suppressed fibrinolysis, loss of natural anticoagulants, and activation of platelets and coagulation factors. Because of these pathophysiologic findings, initial studies started to look for deep venous thrombosis, arterial thrombosis, and microthrombosis. The available data on thrombotic risk are quite limited and based largely on case series from China [123], the Netherlands [6], and France [124]. Recent studies have described a high incidence of deep venous thrombosis and pulmonary embolism varying from 35 to 78% in COVID-19 patients [5, 125, 126].
Nonetheless, most experts agree that the signal for increased thrombotic risk is sufficient to recommend pharmacologic venous thromboembolism (VTE) prophylaxis in all hospitalized COVID-19 patients as long as there is no contraindication [28, 127]. What remains to be confirmed is the real role of therapeutic anticoagulation in these patients. There is much controversy about this issue, while RCT results are not available [16, 128]. The guidelines specifically mention that the anticoagulation regimens may be modified based on extremes of body weight (50% increase in dose if obese), severe thrombocytopenia, or worsening renal function [129].
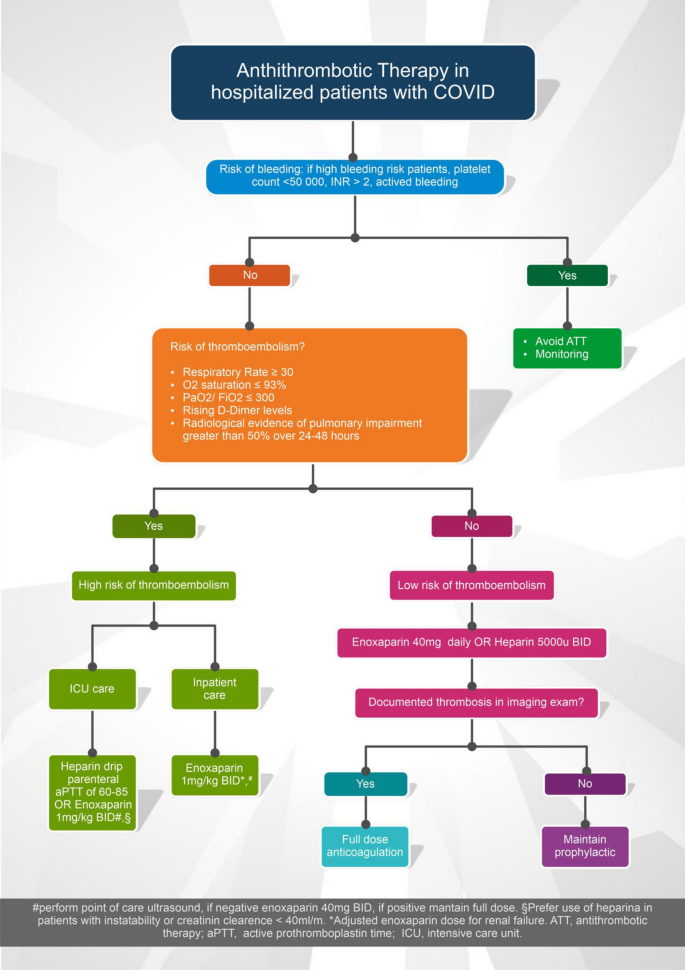
One of the difficulties in determining the true incidence of thrombosis is that access to diagnostic testing may be limited. In a report from the Netherlands (where routine VTE prophylaxis is given), high rates of VTE were noted among ICU patients [6]. More than one-third of these patients, however, had a pulmonary embolism limited to subsegmental. The therapeutic dose should be considered for patients with severe COVID-19 and signs of 1 sepsis-induced coagulopathy (SIC) and/or high D-dimer (6 × higher the reference values) in association with other biomarkers of severity, in the absence of contraindication for anticoagulation. This can be considered a therapeutic strategy for SARS-CoV-2 infection, based on experts’ opinion and a few retrospective studies [15, 16]. Moreover, this strategy requires the use of strict institutional protocols that enable surveillance and rapid intervention if complications occur. Figure 4 shows a proposed algorithm to assess thrombogenesis in patients with COVID-19, as well as a treatment suggestion. However, data are still insufficient to identify critical aspects relevant to therapeutic plans, such as the best drug choice, its dosage, and administration time schedule, as well as the duration of treatment.
Fig. 4
Algorithm proposed for the management of antithrombotic therapy in patients with COVID-19
Full size image Ethical dilemma during the pandemics
The COVID-19 epidemic requires an increased number of resources, reinforcement of the ICU teams with new staff members, reorganization of the unit, and protocol changing. All of these might create vulnerability and loss of control for all the professionals. In many times, intensivists should make their choices based on local politics, structural resources, and team abilities [130].
Conclusions
COVID-19 is one of the most challenging health emergencies we have faced this century. Health professionals are experiencing very difficult times, with limitations of resources and information, which when available needs to be confirmed before integration into clinical practice. To date, there is no proven specific treatment for the management of COVID-19, although studies with promising results have recently emerged. We know already that the lowest rates of mortality are related to better quality of care. Early diagnosis, application of effective therapies and adequate strategies of clinical stratification are needed for better outcomes in COVID-19 patients. We have learned that COVID-19-related respiratory dysfunction has unique characteristics that require individualized management and are aware of the importance of supporting the patients’ hemodynamics because of the high risk of cardiovascular and renal complications. The long duration of this disease poses a challenge for the health system and health professionals. Validated protocols 1 of care are essential when dealing with millions of affected people in different countries and in different levels of care. Until an effective vaccine is widely available, the world will need to adapt to the reality of a pandemic that has come to change all paradigms of modern medicine.
the thing about viruses is that the are communicable. its the rate of trasmission that is dangerous, covid is upwards of 1:3 where each person shedding the virus can infect 3 people. (Vaccinated people are less likely to become infected with a viral load that is that contagious). And then there is the problem of hospitals being overwhelmed with acutely ill covid patients. That happens, and when it does people die because covid patients need specialized care...more attention. All this has been written about and reported extensively but many many people willfully ignore these reports. In my city I have personally heard accounts from doctors and nurses in hospital who lost patients that would otherwise have lived had they not been so busy with other desperately sick people.
I take your points and I certainly know you are sincere. Again, this is not for a pissing contest. There are those that contend and suggest they can prove that the vaccinated are actually carrying a higher viral load and are shedding more than the unvaccinated. I certainly take your point about over over whelmed hospitals. The situation where Florida was being reported as over whelmed was pure fiction. Also if that is indeed a serious concern...why then are they firing or allowing large numbers of medical staff to leave? An accomodation can't be worked out? Does it not make you at least pause that those INVOLVED and in a lot of cases on the front lines don't want anything to do with the vaccine?
I suggest again that there were and are alternative medications that could reduce the death rate.
For adults with COVID-19 and shock, the Panel recommends using dynamic parameters, skin temperature, capillary refilling time, and/or lactate levels over static parameters to assess fluid responsiveness (BIIa).
For the acute resuscitation of adults with COVID-19 and shock, the Panel recommends using buffered/balanced crystalloids over unbalanced crystalloids (BIIa).
For the acute resuscitation of adults with COVID-19 and shock, the Panel recommends against the initial use of albumin for resuscitation (BI).
For adults with COVID-19 and shock, the Panel recommends norepinephrine as the first-choice vasopressor (AI).
For adults with COVID-19 and shock, the Panel recommends titrating vasoactive agents to target a mean arterial pressure (MAP) of 60 to 65 mm Hg over higher MAP targets (BI).
The Panel recommends against using hydroxyethyl starches for intravascular volume replacement in patients with sepsis or septic shock (AI).
When norepinephrine is available, the Panel recommends against using dopamine for patients with COVID-19 and shock (AI).
As a second line vasopressor, the Panel recommends adding either vasopressin (up to 0.03 units/min) (BIIa) or epinephrine (BIIb) to norepinephrine to raise MAP to target or adding vasopressin (up to 0.03 units/min) (BIIa) to decrease norepinephrine dosage.
The Panel recommends against using low-dose dopamine for renal protection (AI).
The Panel recommends using dobutamine in patients who show evidence of cardiac dysfunction and persistent hypoperfusion despite adequate fluid loading and the use of vasopressor agents (BIII).
The Panel recommends that all patients who require vasopressors have an arterial catheter placed as soon as practical, if resources are available (BIII).
For adults with refractory septic shock who have completed a course of corticosteroids to treat their COVID-19, the Panel recommends using low-dose corticosteroid therapy (“shock-reversal”) over no corticosteroid therapy (BIIa).
Oxygenation and Ventilation
For adults with COVID-19 and acute hypoxemic respiratory failure despite conventional oxygen therapy, the Panel recommends high-flow nasal cannula (HFNC) oxygen over noninvasive positive pressure ventilation (NIPPV) (BIIa).
In the absence of an indication for endotracheal intubation, the Panel recommends a closely monitored trial of NIPPV for adults with COVID-19 and acute hypoxemic respiratory failure and for whom HFNC is not available (BIIa).
For patients with persistent hypoxemia despite increasing supplemental oxygen requirements in whom endotracheal intubation is not otherwise indicated, the Panel recommends considering a trial of awake prone positioning to improve oxygenation (CIIa).
The Panel recommends against using awake prone positioning as a rescue therapy for refractory hypoxemia to avoid intubation in patients who otherwise meet the indications for intubation and mechanical ventilation (AIII).
If intubation becomes necessary, the procedure should be performed by an experienced practitioner in a controlled setting due to the enhanced risk of exposing health care practitioners to SARS-CoV-2 during intubation (AIII).
For mechanically ventilated adults with COVID-19 and acute respiratory distress syndrome (ARDS):
The Panel recommends using low tidal volume (VT) ventilation (VT 4–8 mL/kg of predicted body weight) over higher VT ventilation (VT >8 mL/kg) (AI).
The Panel recommends targeting plateau pressures of <30 cm H2O (AIIa).
The Panel recommends using a conservative fluid strategy over a liberal fluid strategy (BIIa).
The Panel recommends against the routine use of inhaled nitric oxide (AIIa).
For mechanically ventilated adults with COVID-19 and moderate-to-severe ARDS:
The Panel recommends using a higher positive end-expiratory pressure (PEEP) strategy over a lower PEEP strategy (BIIa).
For mechanically ventilated adults with COVID-19 and refractory hypoxemia despite optimized ventilation, the Panel recommends prone ventilation for 12 to 16 hours per day over no prone ventilation (BIIa).
The Panel recommends using, as needed, intermittent boluses of neuromuscular blocking agents (NMBA) or continuous NMBA infusion to facilitate protective lung ventilation (BIIa).
In the event of persistent patient-ventilator dyssynchrony, or in cases where a patient requires ongoing deep sedation, prone ventilation, or persistently high plateau pressures, the Panel recommends using a continuous NMBA infusion for up to 48 hours as long as patient anxiety and pain can be adequately monitored and controlled (BIII).
For mechanically ventilated adults with COVID-19, severe ARDS, and hypoxemia despite optimized ventilation and other rescue strategies:
The Panel recommends using recruitment maneuvers rather than not using recruitment maneuvers (CIIa).
If recruitment maneuvers are used, the Panel recommends against using staircase (incremental PEEP) recruitment maneuvers (AIIa).
For critically ill patients with COVID-19 who have acute kidney injury and who develop indications for renal replacement therapy, the Panel recommends continuous renal replacement therapy (CRRT), if available (BIII).
If CRRT is not available or not possible due to limited resources, the Panel recommends prolonged intermittent renal replacement therapy rather than intermittent hemodialysis (BIII).
Pharmacologic Interventions
In patients with COVID-19 and severe or critical illness, there is insufficient evidence for the Panel to recommend either for or against empiric broad-spectrum antimicrobial therapy in the absence of another indication.
If antimicrobials are initiated, the Panel recommends that their use should be reassessed daily to minimize the adverse consequences of unnecessary antimicrobial therapy (AIII).
Extracorporeal Membrane Oxygenation
There is insufficient evidence for the Panel to recommend either for or against the use of extracorporeal membrane oxygenation for patients with COVID-19 and refractory hypoxemia
Again points taken however, o2b and myself are trying to suggest that with Ivermectin and or hydrochloriquine a lot of that could be avoidable. And o2b is correct "they" know the alternatives work.
What is the point of demonizing Dr. Fauci? Hundreds of thousands are dead, more dying daily.
wear your mask...get vaccinated, and find something better to do with your energy
I read half of it; the "monologue" conflates real facts with obvious falsifications, doing so cleverly by using a lot of highly technical language instead of being more accessible. I have numerous counterexamples to these assertions I've seen with my own eyes to indicate to me that this doesn't "fit".
The biggest red flag is the lack of humility and humanity in the writing. Real scientists tend to not speak in such absolutes about EVERYTHING (since there is a lot of nuance to science) and are much more up front about what is known and what isn't. Even published papers are generally clear to state that the respective findings are in scope of their own studies, an acknowledgment that science is about collective consensus over time.
Have you asked yourself why you aren't approaching this overly didactic language with skepticism? Is it possible it's only because it positions itself against what you distrust, i.e. "the enemy of my enemy is my friend?"
Have you considered talking to someone down to earth that can explain all of this in non-science terms and is willing to acknowledge the extent and shortcomings of their own information?