A few very well written articles and studies on pain acceptance.
Which is actually a highly unnatural thing to do...but has shown to be very effective in the reduction of depression/anxiety and pain itself.
Just a few of the things I have been reading through for my presentation next week.
Enjoy!
Accept Your Pain; It Will Hurt Less
Accepting reality leads to change like denial never can.
You are upset—understandably upset—about a difficult situation or some aspect of yourself.
You angrily question how unfair life is or why you don’t change.
You fight the current situation, bringing on feelings of distress about your pain.
This dilemma is so common that the Buddhists long ago reduced it to a formula: Pain x Resistance = Suffering.
Translation: Fighting against (or resisting) the reality of the pain in your life creates suffering.
One common form of resistance is people rejecting their emotions.
For instance, a husband might resist feeling angry towards his wife, though the
anger is genuinely there.
So, he experiences an inner conflict about his anger—on top of continuing to feel angry.
It’s not unusual for people to be critical of their emotions when they think they are wrong for feeling a particular way.
However,
emotions can’t be wrong—they just are.
Saying your emotions are wrong is like saying you were born with the wrong color hair.
You might prefer to be a blonde (something you
can change—at least temporarily—with a bottle), but that doesn’t mean it’s wrong to be a brunette.
Similarly, the husband feels angry, which is neither right nor wrong.
Another common form of resistance occurs when people are critical of inherent traits.
For instance, I have treated a number of anxious introverts who struggle with not liking parties.
They think there is something wrong with themselves for this (a judgment that is supported by Western culture).
But, there is nothing inherently wrong with being introverted—it even has its benefits, such as sometimes being able to develop more intimate (though fewer) relationships.
Rather than resisting your pain, and so creating your own suffering, you would be
wise to learn to accept your
authentic self—your experience of who you really are and what you are really struggling with.
In doing this, you can develop self-acceptance and
self-compassion.
For instance, when the introvert accepts her
introversion, she can feel good about herself; whether or not she decides to work on developing more social interactions.
She can also be compassionate to her own struggles with attending parties.
People who live authentically act in keeping with their inner experiences—such as their likes, dislikes, interests and values.
They are happier in their relationships and achieve a greater sense of inner peace.
You can experience this, too, by doing the following:
Begin by accepting your current reality.
Your situation is what it is.
No amount of wishing for something different or rejecting the situation (or yourself) will change anything.
However, by facing your problem, you can at least begin to address it.
Pay attention to your thoughts, feelings, and desires.
Only by knowing your inner experiences can you be true to them.
When they are painful, you can then at least find ways to comfort yourself and cope as effectively as possible with them.
Choose to be accepting and compassionate to your experiences.
No one ever healed from a blow to the head by hitting themselves there again.
The same can be said of emotional pain; that is, self-criticism about some difficulty won’t resolve that problem.
In both cases, the way to heal and move beyond the hurt is to accept it and find ways to nurture the wound.
More specifically with psychological pain, acceptance and compassion are essential to heal and to free yourself to nurture greater personal growth.
Plan for a better future.
If you are unhappy with some aspect of yourself or your circumstance, you would benefit from planning for the change you would like to see—even as you accept and nurture your current self.
Develop supportive friendships.
No one gets through this world alone.
At some time or another, we all go through rough patches in life and can benefit from the support of good, caring friends.
In short, by accepting the present and having compassion for yourself, you can soothe your pain as you create a happier, more fulfilling future.
Leslie Becker-Phelps, Ph.D. is a clinical psychologist in private practice and is on the medical staff at Somerset Medical Center in Somerville, NJ. She also writes a blog for WebMD (
The Art of Relationships) and is the relationship expert on
WebMD’s Relationships and Coping Community.
_______________________________________________________________________________________________________________
A really great study...I have posted the summary but there is a lot of very good information within the complete study you can find here:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2671308/
The meaning and process of pain acceptance.
Perceptions of women living with arthritis and fibromyalgia.
Within the past 10 years, cognitive-behavioural pain management models have moved beyond the traditional focus on coping strategies and perceived control over pain, to incorporate mindfulness-and acceptance-based approaches.
Pain acceptance is the process of giving up the struggle with pain and learning to live life despite pain.
Acceptance is associated with lower levels of pain, disability and psychological distress.
Relatively little is known, however, about how patients arrive at a state of acceptance without the aid of therapy.
OBJECTIVES:
To explore personal definitions of acceptance and the factors that facilitate or hinder acceptance.
METHODS:
Eleven focus groups, involving a total of 45 women with arthritis and fibromyalgia, were conducted.
RESULTS:
The qualitative analysis revealed that, while the women rejected the word ‘acceptance’, they did agree with the main components of existing research definitions.
The women’s responses revealed that acceptance was a process of realizations and acknowledgements, including realizing that the pain was not normal and help was needed, receiving a diagnosis, acknowledging that there was no cure and realizing that they needed to redefine ‘normal’.
Diagnosis, social support, educating self and others, and self-care were factors that promoted acceptance.
Struggling to retain a prepain identity, negative impacts on relationships, others not accepting their pain and the unspoken message that the pain was ‘all in their head’ were barriers to acceptance.
CONCLUSION:
The implications of these findings, distinctions between the diagnostic groups and recommendations regarding how health professionals can facilitate the process of acceptance are discussed.
The experience of persistent pain prompts a search for understanding that initially focuses on diagnosis and treatment recommendations that will eliminate the pain.
When initial attempts are unsuccessful, patients often undertake a vigorous quest to find a cure (
1).
This search can dominate a person’s life, leading him or her to try a variety of pharmacological, physical and ‘alternative’ therapies (
2).
When the pain experience continues, however, he or she is confronted with the reality of ‘learning to live with’ chronic pain (
1,
3,
4).
Consistent with this reality, researchers and clinicians in the cognitive-behavioural tradition have begun to embrace mindfulness- and acceptance-based approaches.
Based on the initial work of Hayes et al (
5,
6), Geiser (
7) and McCracken et al (
1,
8–
10) extended the acceptance-based approach to persons with chronic pain.
In this context, acceptance is generally viewed as “a willingness to experience continuing pain without needing to reduce, avoid, or otherwise change it” (
8).
Factor analysis of the main tool for measuring acceptance – the Chronic Pain Acceptance Questionnaire (CPAQ) – reveals four components:
“(
1) activity engagement (pursuit of life activities regardless of pain); (
2) pain willingness (recognition that avoidance and control are often unworkable methods of adapting to chronic pain); (
3) thought control (belief that pain can be controlled or changed by altering one’s thoughts); and (
4) chronicity (recognizing that pain may not change)” (
9).
Based on evaluation of the psychometric properties of these four subscales, however, McCracken et al (
9) reduced the CPAQ to only two subscales (activity engagement and pain willingness).
Acceptance has emerged as a valuable construct in understanding adjustment.
Using correlational designs, researchers demonstrated that acceptance is associated with better physical, social and emotional functioning (
1,
11,
12).
Furthermore, in clinical studies (
1,
7,
10,
13,
14), researchers demonstrated that increased acceptance is associated with improvements in physical, social and emotional functioning, in work-related functioning, and in analgesic and health care use.
Despite the demonstrated benefits of acceptance, relatively little is known about how patients typically arrive at a state of acceptance when they do not undergo a formal acceptance-and commitment-based therapy (ACT) program.
Although several studies have examined the general process of adjustment (
15–
17) and researchers are delineating how ACT can promote acceptance (
5,
6), no study, to our knowledge, has investigated the meaning or process of pain acceptance outside of therapy.
In a related study, Risdon et al (
18) identified eight accounts of the meaning of acceptance among 30 individuals from the community (the mean age of participants was 46 years and the majority were women, but no further descriptive data regarding the sample characteristics were provided).
The eight accounts identified were taking control, living day-to-day, acknowledging limitations, empowerment, accepting loss of self, acknowledging that there is more to life than pain, relinquishing the fight against battles that cannot be won and reliance on spiritual strength.
However, only five of these participants identified themselves as having chronic pain.
The intent of the present study was to examine the meaning and process of pain acceptance for individuals who have not participated in an ACT program.
It is important to investigate the process of acceptance outside of therapy because the vast majority of persons with chronic pain never participate in formalized psychotherapy.
__________________________________________________________________________________________________________________
What is Acceptance of Pain and Why Would Anyone Want it?
Over recent decades, a reasonable amount of data has been generated which suggests that greater acceptance of chronic pain is associated with fewer pain-related difficulties, such as distress and disability, and better overall quality of life (for reviews, see: McCracken & Vowles, 2014; Scott & McCracken, 2015; Vowles & Thompson, 2011).
Pragmatically, however, the idea that one might want to be more “accepting” of chronic pain runs contrary to common sense and may be confusing.
It may also lead to people with pain simply being told to “accept it,” which generally fails to do much of anything useful.
Part of the confusion surrounding acceptance may arise from the history behind behavioral approaches to health as they compare to modern approaches that often prioritize the reduction or elimination of undesirable personal experiences such as pain.
Part of the confusion likely also comes from the paradoxical nature of acceptance in relation to these undesirable experiences.
Acceptance by itself is unnatural.
Thus, “accepting it” is probably not the whole story – it is necessary to also identify the purpose of acceptance.
My hope for this blog is to provide clarity in relation to the potential areas for confusion regarding the proposed role and purpose of acceptance as it pertains to chronic pain.
An accurate understanding of acceptance in chronic pain requires some history.
The study of acceptance can trace its roots back to the radical, or “thoroughgoing,” behaviorism of Skinner (Skinner, 1945, 1974; also see Moore, 2008 for an outstanding book-length exposition on radical behaviorism).
Skinner’s work has two important facets as it relates to why greater acceptance of pain might be useful.
The first is that the radical behavioral tradition views strictly eliminative approaches, those which prioritize the elimination of behavior or symptoms, and are therefore based in aversive control (Follette, Linnerooth, & Ruckstuhl, 2001; Lovibond, 1970), as highly problematic.
The problem with these approaches stems principally from the fact that aversive control leads to a narrowing of response options, which generally function as attempts to avoid or escape from the aversive experience, as well as an insensitivity to the relation between behavior and its consequences (Goldiamond, 1974; Hawkins, 1986).
In chronic pain, for example, response options to pain can narrow such that the dominant mode of responding is one of pain avoidance – the person’s life is dominated by efforts to avoid or eliminate pain.
The literature is replete with data suggesting that such inflexible avoidance brings with it broader negative consequences in the form of worsening and sustained disability and distress.
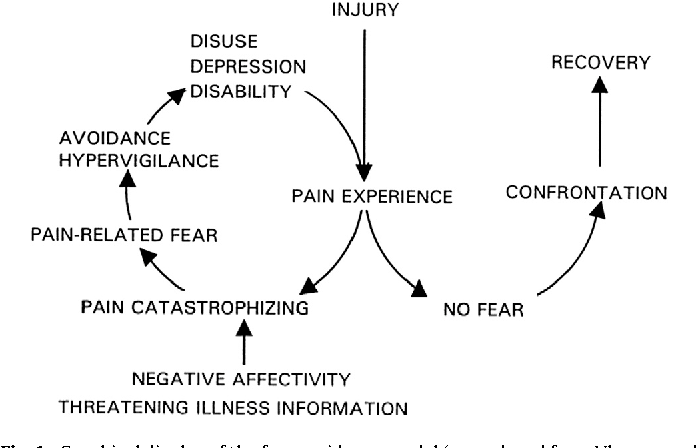
The well-established fear avoidance model of pain (Leeuw et al., 2007; Lethem, Slade, Troup, & Bentley, 1983; Vlaeyen & Linton, 2000) represents a prime example focusing the deleterious impact of persistent avoidance on functioning.
From the perspective of radical behaviorism, the problem here is not limited to avoidance and its associated problems, further problems are likely when avoidance behavior persists in spite of equally persistent failures to achieve its objective (i.e., pain reduction or elimination) over the longer term.
Spending the day in bed to avoid pain simply doesn’t work for those who have chronic pain.
The pain returns.
Pushing through the “pain barrier” doesn’t work – because beyond that barrier is more pain.
In other words, pain persists in spite of persistent behavior to avoid it.
Persistent pain unwillingness, the antithesis of pain acceptance, may likewise reflect maladaptive behavior control efforts and indicate an insensitivity, or lack of responsiveness, to the equally persistent failing quality of the respondent behavior.
Thus, excessive aversive control can lead to problems – avoidance attempts dominate as the goal is to avoid the aversive sensation of pain, these avoidance attempts fail as pain continues, and life becomes smaller and more limited for the person in pain.
Aversive control can be contrasted with appetitive control.
It may be most helpful to define this latter term in relation to an example treatment approach based in Skinner’s radical behaviorism, that of Acceptance and Commitment Therapy (ACT; Hayes, Strosahl, & Wilson, 2012).
As part of its stated success criteria for chronic pain, ACT does not require elimination, or even reduction, of pain – or other aversive experiences for that matter (see Vowles, 2015 for an introduction to a special issue on this topic) – for treatment success.
It isn’t that ACT practitioners don’t want people to feel better, it’s that it isn’t a prerequisite for treatment success.
ACT focuses neither on the elimination of experiences or symptoms, nor on making use of aversive control.
Instead, it aims to build behavioral repertoires that effectively achieve positive goals over the long term.
The intended purpose is an increase in consistent and reliable engagement in valued activities with pain, both when it is low but also when it isn’t.
This non pain-contingent process relies on one of appetitive control over behavior, behavior that is directed towards the pursuit of what is desired.
These two aspects of control, aversive and appetitive, have particular relevance with regard to the goals of treatment.
If a lack of acceptance is indeed a reflection of wide-spread aversive control over an individual’s behavior, then perhaps treatments which are predominantly reliant on aversive control themselves, in this case treatments that focus only or primarily on pain reduction, may be ill-advised in a context of significant unwillingness to experience pain.
Perhaps paradoxically, significant unwillingness may signal a need for increased willingness in the service of valued activities, not less pain, better pain “management”, or other similar interventions.
In essence, what may be needed is appetitive control – the pursuit of activities that have importance, meaning, and value even with ongoing pain.
Thus, the issue is not to just “accept it”, but to determine if there are areas in life that are worth the experience of pain.
In my clinical experience, people with pain can readily identify these areas, desperately want to return to them, and readily agree that these areas matter even when pain is present.
Such patient sentiments can allow further conversations about whether treatment might usefully include valued areas and progress towards them as a marker of treatment success.
To summarize, from one perspective, the purpose of treatment is to allow patients to engage in activities that allow for a quality of life sufficient for their needs.
It is within this purpose that acceptance of pain can be relevant – sometimes greater acceptance of, and consequently less time and energy spent struggling and avoiding, pain may free up behavior to allow for the pursuit of what is valued.



")



")