
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
The Lack of Affordable Healthcare in the US
- Thread starter Skarekrow
- Start date
-
- Tags
- healthcare obamacare trumpcare
More options
Who Replied?Skarekrow
~~DEVIL~~
- MBTI
- Ni-INFJ-A
- Enneagram
- Warlock
They are all true!I won't lie, the healthcare system in the US is the primary reason why I'm reticent about the idea of moving to that country.
Some of the stories you've shared have sent shivers down my spine, Skare.
No shit.
1. Medical bills are the number one reason for bankruptcy in the United States, causing more than 60% of all BK’s. Approximately three-fourths of those who go BK because of medical bills have health insurance.
2. An illness or hospital stay that requires intensive care can easily rack up medical bills over one million dollars.
3. Every year, it’s estimated that hospitals overcharge Americans by about 10 billion dollars.
4. Medical billing advocates estimate that over 90% of the medical bills thy audit have “gross overcharges.”
5. 41% of working age Americans are currently paying off medical debt or have some sort of medical bill problems.
6. Hospitals often knock their bills down by 95% for those who know their system and how it works, but the uninsured, uneducated, and secondary language speakers often have no access to these discounts.
7. The average recovery on hospital medical bills is 15.3%. Non-hospital medical facilities recover an average of 21.8% of each bill.
8. U.S. hospitals write off about 5.4% of their gross revenue as bad or unrecoverable patient debt every quarter.
9. In 2012, 75 million people reported having problems paying off their medical debt, up from only 58 million in 2005.
10. The average uninsured household has zero assets.
11. At least 24 pharmaceutical companies made over a billion dollars profit in 2008, alone.
12. Litigation and liability in the medical system added an estimated $55.6 billion to healthcare costs in 2008 alone.
13. Americans spend about 200% for healthcare compared to people in other developed nations, but receive much lower quality and efficiency.
14. The foreign-born population was about two-and-a-half times more likely to be without health insurance than those born in the U.S.
15. The uninsured end up paying for 35% of their care out-of-pocket. They are typically billed more and pay more than insured patients.
16. More than 80% of uninsured are U.S. citizens and 19.7% are non-citizens.
17. More than 60% of the uninsured have at least one full-time worker in their family, and 16% have at least one part-time worker.
18. 28% of adults with a chronic health condition say they’ve skipped doses or didn’t fill a prescription because of the cost.
19. In 2012, 43% of adults, or 80 million people, skilled or delayed needed medical care because of the cost.
20. That includes 26.8% of families that have experienced the financial burden of trying to pay medical bills.
21. Almost 1 in 6, or 16.5%, of U.S. families had trouble paying medical bills within the last 12 months.
22. More than one in three, or 36% of families with children experience financial burdens due to medical care.
23. More than 1 in 5 families, or 21.4%, were trying to pay their medical bills over time.
24. Approximately 15.4% of the U.S. population was without health insurance in 2012, or 48.6 million people.
25. In 2012, Health care spending in the United States grew 3.7% to $2.8 trillion, or $8,915 per person.
26. Between 1999 and 2009, health insurance premiums for small employers increased by 180%.
27. U.S. wages increased by 3.8% between 2000 and 2006, but health care cost premiums increased by 87%.
28. Even during the Great Recession, U.S. healthcare companies cashed in, increasing their profits by 56% just in 2009.
29. The five biggest for-profit health insurance companies in the U.S. made a combined profit of $12.2 billion just in 2009.
30. The top executives at those five companies made $200 million in compensation that year.

Last edited:
JennyDaniella
Stargazer
- MBTI
- INFJ
- Enneagram
- 925
This is one of the many reasons why I opted out being a physician despite having such a great passion in the sciences. I can't imagine being a physician and having to deal with crooked individuals that are involved in the big pharma. While I do appreciate the works, integrity and passion that some doctors instill in their medical careers and try to be compassionate for their patients---there is no doubt that other doctors are in it for the money as well. Prescribing patients with prescription pills is an automatic chunk of money---or even surgery and treatments.
It disgusts me how the American healthcare system works, absolutely infuriates me. Luckily, being a clinical neuropsychologist won't require me to prescribe my patients any medicine but rather actually counsel others and research on the side.
The more I look into the big phrama and their involvement in other fishy situations such as the opioid epidemic that is going around, the more I am shocked. Smh. Ridiculous. The lack of human kindness and integrity is almost non-existent.
It disgusts me how the American healthcare system works, absolutely infuriates me. Luckily, being a clinical neuropsychologist won't require me to prescribe my patients any medicine but rather actually counsel others and research on the side.
The more I look into the big phrama and their involvement in other fishy situations such as the opioid epidemic that is going around, the more I am shocked. Smh. Ridiculous. The lack of human kindness and integrity is almost non-existent.
- MBTI
- INFJ
- Enneagram
- 954 so/sx
I propose a machine of whirling cheese graters!
Shit got real in this thread
JennyDaniella
Stargazer
- MBTI
- INFJ
- Enneagram
- 925
Skarekrow
~~DEVIL~~
- MBTI
- Ni-INFJ-A
- Enneagram
- Warlock
This is one of the many reasons why I opted out being a physician despite having such a great passion in the sciences. I can't imagine being a physician and having to deal with crooked individuals that are involved in the big pharma. While I do appreciate the works, integrity and passion that some doctors instill in their medical careers and try to be compassionate for their patients---there is no doubt that other doctors are in it for the money as well. Prescribing patients with prescription pills is an automatic chunk of money---or even surgery and treatments.
It disgusts me how the American healthcare system works, absolutely infuriates me. Luckily, being a clinical neuropsychologist won't require me to prescribe my patients any medicine but rather actually counsel others and research on the side.
The more I look into the big phrama and their involvement in other fishy situations such as the opioid epidemic that is going around, the more I am shocked. Smh. Ridiculous. The lack of human kindness and integrity is almost non-existent.
I felt similarly while working for certain hospitals.
Some were really great and very patient-centric...but many more and growing were the for-profit human farms, where they milk your cash while you are sick and have no choice.
Yes...I have thoughts about the opioid “crisis”.
Those very same doctors who get folks addicted offer them no way to become un-addicted that isn’t hellacious and terrible.
So then people turn to street drugs with norfentanyl from China in it OD’ing people.
Though...there are those like myself who have been on pain meds for many many years and have never let the medications get the better of them and have always maintained without turning to illegal narcotics - this just makes it all the more difficult for those who truly need the medications, have never abused them, and help keep people functional and not suicidal from chronic pain.
So both of those things piss me off...all the while big pharma is making a killing.
Literally and figuratively.
It is quite sad I concur.
Damn skippy!Shit got real in this thread
Last edited:
Skarekrow
~~DEVIL~~
- MBTI
- Ni-INFJ-A
- Enneagram
- Warlock
Crazy that our system is so unbalanced and flat out screwed up.
If you are poor or not white...you get treated even worse here in the US.
Examples of Cancer Health Disparities

Cancer affects people of all races and ethnicities in the U.S.; however, the burden is greater for certain populations. Below are selected statistics that illustrate the impact of cancer health disparities by socioeconomic status, racial/ethnic group, and cancer type.
Cancer Disparities by Socioeconomic Status and Medically Underserved Populations
African Americans
Disparities by Cancer Type
Breast
If you are poor or not white...you get treated even worse here in the US.
Examples of Cancer Health Disparities

Cancer affects people of all races and ethnicities in the U.S.; however, the burden is greater for certain populations. Below are selected statistics that illustrate the impact of cancer health disparities by socioeconomic status, racial/ethnic group, and cancer type.
Cancer Disparities by Socioeconomic Status and Medically Underserved Populations
- People with lower socioeconomic status (SES) have disproportionately higher cancer death rates than those with higher SES, regardless of demographic factors such as race/ethnicity. (American Cancer Society-ACSExit Disclaimer)
- Studies have found that SES factors are associated with an individual’s or group’s risk of developing and surviving cancer— more than race or ethnicity. SES factors include access to education, certain occupations, health insurance, and living conditions—including exposure to environmental toxins.
- SES appears to play a major role in influencing the prevalence of behavioral risk factors for cancer (for example, tobacco smoking, physical inactivity, obesity, excessive alcohol intake, and health status), as well as in following cancer screening recommendations.
- Individuals from medically underserved populations are more likely to be diagnosed with late-stage diseases that might have been treated more effectively or cured if diagnosed earlier.
African Americans
- For all cancers combined, cancer incidence rates between 2007 through 2011 were the highest overall in black men (587.7 per 100,000 men) compared to any other racial or ethnic group. (NCI)
- African Americans have the highest mortality rate of any racial or ethnic group for all cancers combined and for most major cancers. (DHHS Office of Minority Health- OMH)
- For all cancers combined, the death rate is 25 percent higher for African Americans/blacks than for whites.
- African American women with cancer have higher death rates despite them having a lower risk of cancer overall (compared to white women). (ACSExit Disclaimer)
- African American men have lower 5-year cancer survival rates for lung, colon, and pancreatic cancers compared to non-Hispanic white men. (DHHS OMH)
- Cancer is the second leading cause of death among Native Americans over age 45. (NCI)
- While overall cancer mortality rates from 2001 through 2010 decreased by 1.4 percent per year among whites and by 2.1 percent per year among African Americans/blacks, they decreased by only 0.7 percent per year among American Indians and Alaska Natives.(NCI)
- American Indians and Alaska Natives continue to have the poorest 5-year survival rates among all racial and ethnic groups, for all cancers combined. (NCI)
- Asian Americans and Pacific Islanders have the highest incidence rates for both liver and stomach cancers and are twice as likely to die from these cancers as whites. This may be caused by a higher prevalence of infections with hepatitis B virus (liver cancer) and the bacterium H. pylori (stomach cancer). (ACSExit Disclaimer)
- Native Hawaiians/Pacific Islanders are 30 percent more likely to be diagnosed with cancer compared to non-Hispanic whites. (DHHS OMH)
- Hispanics and Latinos have the highest rates for cancers associated with infection, such as liver, stomach, and cervical cancers. Higher prevalence of infection with human papillomavirus (cervical cancer), hepatitis B virus (liver cancer), and the bacterium H. pylori (stomach cancer) in immigrant countries of origin contributes to these disparities. (ACSExit Disclaimer)
- Although Hispanics and Latinos have lower incidence and death rates for the most common cancers than non-Hispanic whites, they are more likely to be diagnosed with advanced stages of disease. (NCI)

Disparities by Cancer Type
Breast
- Where breast cancer rates stabilized between 2002 and 2011 in non-Hispanic white women, rates continue to increase among African American/black women. (JNCIExit Disclaimer)
- African American/black women are more likely to die from breast cancer despite white women having higher incidence rates for the disease.
- African American women are almost 40 percent more likely to die from breast cancer compared to non-Hispanic white women. (DHHS OMH)
- African American women with breast cancer are less likely than white women to survive five years after diagnosis. The survival rate among African American women is 71 percent, compared to 86 percent among whites. (JNCIExit Disclaimer)
- Recent NCI-supported research indicates that aggressive breast tumors are more common in younger African American/black and Hispanic/Latino women living in low SES areas. This more aggressive form of breast cancer is less responsive to standard cancer treatments and is associated with poorer survival.
- Rates for triple-negative breast cancers (HR-/HER2-) were highest among non-Hispanic black women compared with all other racial/ethnic groups with an age-adjusted rate of 27.2 per 100,000 women; a rate 1.9 times higher than the non-Hispanic white rate, 2.3 times higher than the Hispanic rate, and 2.6 times higher than the non-Hispanic API (NHAPI) rate. (JNCIExit Disclaimer)
- Overall, compared with non-Hispanic white women, African American/black women are screened less frequently for breast cancer, are more likely to have advanced disease when a diagnosis is made, have a poorer prognosis for a given stage of disease, and have less access to medical care. (NCI)
- African American/black women are more likely to be diagnosed with cervical cancer compared to white women in the general U.S. population.
- Despite recent declines in cervical cancer overall, African American women with cervical cancer have higher mortality rates than women of any other racial or ethnic group in the United States.
- Hispanic women are almost twice as likely to have cervical cancer and 1.4 times more likely to die from cervical cancer as compared to non-Hispanic white women. (DHHS OMH)
- The disproportionate burden of cervical cancer in Hispanic/Latino and African American women is primarily due to a lack of screening.
- Among Asian Americans, incidence rates for cervical cancer are almost three times higher in Vietnamese women than in Chinese and Japanese women. (ACSExit Disclaimer)
- African Americans have higher mortality rates and higher incidence rates of colorectal cancer than all other racial/ethnic groups, except American Indians/Alaska Natives.
- Kidney cancer incidence and mortality rates are twice as high in men as in women.
- American Indians/Alaska Natives have higher kidney cancer incidence and mortality rates than any other racial/ethnic groups in the United States.
- American Indian/Alaska Native women are 40 percent more likely to have kidney/renal pelvis cancer than non-Hispanic white women. (DHHS OMH)
- The incidence rates of liver cancer for Asian American/Pacific Islander men and women are 2.4 and 2.7 times greater, respectively, than those of non-Hispanic white men and women. (DHHS OMH)
- Both Hispanic men and women are twice as likely to be diagnosed with and to die from liver cancer compared to non-Hispanic whites. (DHHS OMH)
- African American/black men and women have the highest incidence of lung cancer compared to the general U.S. population.
- Mortality rates from lung cancer are highest among African American males than other population groups.
- African Americans have approximately twice the incidence and mortality rates of multiple myeloma than the general U.S. population.
- African Americans have higher rates of pancreatic cancer incidence and mortality than any other racial or ethnic group.
- One in five (20 percent) African American men will be diagnosed with prostate cancer during their lifetime. (ACSExit Disclaimer)
- African American men have the highest incidence rate for prostate cancer in the U.S. and are more than twice as likely as white men to die of the disease. (NCI)
- Prostate cancer is the second leading cause of cancer-related deaths among African American men. (ACSExit Disclaimer)
- Incidence rates of stomach cancer are highest in American Indians/Alaska Natives, followed by Hispanics/Latinos, Asian Americans/Pacific Islanders, and African Americans. (ACSExit Disclaimer)
- Mortality rates from stomach cancer are highest in Asian Americans/Pacific Islanders and African Americans, followed by Hispanics/Latinos, American Indians/Alaska Natives, and whites.
- African American women are 2.4 times as likely to be diagnosed with stomach cancer, and 2.5 times as likely to die from stomach cancer, compared to non-Hispanic white women. (DHHS OMH)
- Asian/Pacific Islander men are twice as likely to die from stomach cancer compared to the non-Hispanic white population, and Asian/Pacific Islander women are 2.7 times as likely to die from the same disease. (DHHS OMH)
- Hispanic women are 2.2 times more likely to have stomach cancer compared to non-Hispanic white women. (DHHS OMH)
JennyDaniella
Stargazer
- MBTI
- INFJ
- Enneagram
- 925
Crazy that our system is so unbalanced and flat out screwed up.
If you are poor or not white...you get treated even worse here in the US.
Examples of Cancer Health Disparities
Cancer affects people of all races and ethnicities in the U.S.; however, the burden is greater for certain populations. Below are selected statistics that illustrate the impact of cancer health disparities by socioeconomic status, racial/ethnic group, and cancer type.
Cancer Disparities by Socioeconomic Status and Medically Underserved Populations
Cancer Disparities by Racial/Ethnic Groups
- People with lower socioeconomic status (SES) have disproportionately higher cancer death rates than those with higher SES, regardless of demographic factors such as race/ethnicity. (American Cancer Society-ACSExit Disclaimer)
- Studies have found that SES factors are associated with an individual’s or group’s risk of developing and surviving cancer— more than race or ethnicity. SES factors include access to education, certain occupations, health insurance, and living conditions—including exposure to environmental toxins.
- SES appears to play a major role in influencing the prevalence of behavioral risk factors for cancer (for example, tobacco smoking, physical inactivity, obesity, excessive alcohol intake, and health status), as well as in following cancer screening recommendations.
- Individuals from medically underserved populations are more likely to be diagnosed with late-stage diseases that might have been treated more effectively or cured if diagnosed earlier.
African Americans
American Indian and Alaska Native
- For all cancers combined, cancer incidence rates between 2007 through 2011 were the highest overall in black men (587.7 per 100,000 men) compared to any other racial or ethnic group. (NCI)
- African Americans have the highest mortality rate of any racial or ethnic group for all cancers combined and for most major cancers. (DHHS Office of Minority Health- OMH)
- For all cancers combined, the death rate is 25 percent higher for African Americans/blacks than for whites.
- African American women with cancer have higher death rates despite them having a lower risk of cancer overall (compared to white women). (ACSExit Disclaimer)
- African American men have lower 5-year cancer survival rates for lung, colon, and pancreatic cancers compared to non-Hispanic white men. (DHHS OMH)
Asian Americans, Native Hawaiians, and other Pacific Islanders
- Cancer is the second leading cause of death among Native Americans over age 45. (NCI)
- While overall cancer mortality rates from 2001 through 2010 decreased by 1.4 percent per year among whites and by 2.1 percent per year among African Americans/blacks, they decreased by only 0.7 percent per year among American Indians and Alaska Natives.(NCI)
- American Indians and Alaska Natives continue to have the poorest 5-year survival rates among all racial and ethnic groups, for all cancers combined. (NCI)
Hispanics/Latinos
- Asian Americans and Pacific Islanders have the highest incidence rates for both liver and stomach cancers and are twice as likely to die from these cancers as whites. This may be caused by a higher prevalence of infections with hepatitis B virus (liver cancer) and the bacterium H. pylori (stomach cancer). (ACSExit Disclaimer)
- Native Hawaiians/Pacific Islanders are 30 percent more likely to be diagnosed with cancer compared to non-Hispanic whites. (DHHS OMH)
- Hispanics and Latinos have the highest rates for cancers associated with infection, such as liver, stomach, and cervical cancers. Higher prevalence of infection with human papillomavirus (cervical cancer), hepatitis B virus (liver cancer), and the bacterium H. pylori (stomach cancer) in immigrant countries of origin contributes to these disparities. (ACSExit Disclaimer)
- Although Hispanics and Latinos have lower incidence and death rates for the most common cancers than non-Hispanic whites, they are more likely to be diagnosed with advanced stages of disease. (NCI)
Disparities by Cancer Type
Breast
Cervical
- Where breast cancer rates stabilized between 2002 and 2011 in non-Hispanic white women, rates continue to increase among African American/black women. (JNCIExit Disclaimer)
- African American/black women are more likely to die from breast cancer despite white women having higher incidence rates for the disease.
- African American women are almost 40 percent more likely to die from breast cancer compared to non-Hispanic white women. (DHHS OMH)
- African American women with breast cancer are less likely than white women to survive five years after diagnosis. The survival rate among African American women is 71 percent, compared to 86 percent among whites. (JNCIExit Disclaimer)
- Recent NCI-supported research indicates that aggressive breast tumors are more common in younger African American/black and Hispanic/Latino women living in low SES areas. This more aggressive form of breast cancer is less responsive to standard cancer treatments and is associated with poorer survival.
- Rates for triple-negative breast cancers (HR-/HER2-) were highest among non-Hispanic black women compared with all other racial/ethnic groups with an age-adjusted rate of 27.2 per 100,000 women; a rate 1.9 times higher than the non-Hispanic white rate, 2.3 times higher than the Hispanic rate, and 2.6 times higher than the non-Hispanic API (NHAPI) rate. (JNCIExit Disclaimer)
- Overall, compared with non-Hispanic white women, African American/black women are screened less frequently for breast cancer, are more likely to have advanced disease when a diagnosis is made, have a poorer prognosis for a given stage of disease, and have less access to medical care. (NCI)
Colorectal
- African American/black women are more likely to be diagnosed with cervical cancer compared to white women in the general U.S. population.
- Despite recent declines in cervical cancer overall, African American women with cervical cancer have higher mortality rates than women of any other racial or ethnic group in the United States.
- Hispanic women are almost twice as likely to have cervical cancer and 1.4 times more likely to die from cervical cancer as compared to non-Hispanic white women. (DHHS OMH)
- The disproportionate burden of cervical cancer in Hispanic/Latino and African American women is primarily due to a lack of screening.
- Among Asian Americans, incidence rates for cervical cancer are almost three times higher in Vietnamese women than in Chinese and Japanese women. (ACSExit Disclaimer)
Kidney
- African Americans have higher mortality rates and higher incidence rates of colorectal cancer than all other racial/ethnic groups, except American Indians/Alaska Natives.
Liver
- Kidney cancer incidence and mortality rates are twice as high in men as in women.
- American Indians/Alaska Natives have higher kidney cancer incidence and mortality rates than any other racial/ethnic groups in the United States.
- American Indian/Alaska Native women are 40 percent more likely to have kidney/renal pelvis cancer than non-Hispanic white women. (DHHS OMH)
Lung
- The incidence rates of liver cancer for Asian American/Pacific Islander men and women are 2.4 and 2.7 times greater, respectively, than those of non-Hispanic white men and women. (DHHS OMH)
- Both Hispanic men and women are twice as likely to be diagnosed with and to die from liver cancer compared to non-Hispanic whites. (DHHS OMH)
Multiple Myeloma
- African American/black men and women have the highest incidence of lung cancer compared to the general U.S. population.
- Mortality rates from lung cancer are highest among African American males than other population groups.
Pancreatic
- African Americans have approximately twice the incidence and mortality rates of multiple myeloma than the general U.S. population.
Prostate
- African Americans have higher rates of pancreatic cancer incidence and mortality than any other racial or ethnic group.
Stomach
- One in five (20 percent) African American men will be diagnosed with prostate cancer during their lifetime. (ACSExit Disclaimer)
- African American men have the highest incidence rate for prostate cancer in the U.S. and are more than twice as likely as white men to die of the disease. (NCI)
- Prostate cancer is the second leading cause of cancer-related deaths among African American men. (ACSExit Disclaimer)
- Incidence rates of stomach cancer are highest in American Indians/Alaska Natives, followed by Hispanics/Latinos, Asian Americans/Pacific Islanders, and African Americans. (ACSExit Disclaimer)
- Mortality rates from stomach cancer are highest in Asian Americans/Pacific Islanders and African Americans, followed by Hispanics/Latinos, American Indians/Alaska Natives, and whites.
- African American women are 2.4 times as likely to be diagnosed with stomach cancer, and 2.5 times as likely to die from stomach cancer, compared to non-Hispanic white women. (DHHS OMH)
- Asian/Pacific Islander men are twice as likely to die from stomach cancer compared to the non-Hispanic white population, and Asian/Pacific Islander women are 2.7 times as likely to die from the same disease. (DHHS OMH)
- Hispanic women are 2.2 times more likely to have stomach cancer compared to non-Hispanic white women. (DHHS OMH)
I actually worked on a project dealing with disparity in my Diversity of Psychology class this semester. SES and race/ethnicity is also strongly correlated with mental health as well. It’s terrible how those from different SES and race/ethnicity backgrounds are treated in the healthcare system and not provided for equally. Mental health services are almost unavailable for those that are non-whites due to insurance not being able to cover for therapy, and the lack of hospitals and clinics nearby due to being in major cities or suburbs. So most of the time in low SES neighborhoods, you see a higher rate of depression, bipolar disorders, anxiety disorders, schizophrenia, and severe addictions to drugs and alcohol.
Also, residential segregation is also a huge part of overall well-being as healthy foods are heavily priced and quite scarce, so you would mostly see a majority of fast-food joints in every heavily Black and Hispanic populated neighborhoods, almost in every corner.
It’s almost as if Black, Hispanic and other non-white group neighborhoods are bound to be in situations that are out of their control, and they end up in positions of extreme illness.
Skarekrow
~~DEVIL~~
- MBTI
- Ni-INFJ-A
- Enneagram
- Warlock
You are right...it is across the whole of healthcare in the US!I actually worked on a project dealing with disparity in my Diversity of Psychology class this semester. SES and race/ethnicity is also strongly correlated with mental health as well. It’s terrible how those from different SES and race/ethnicity backgrounds are treated in the healthcare system and not provided for equally. Mental health services are almost unavailable for those that are non-whites due to insurance not being able to cover for therapy, and the lack of hospitals and clinics nearby due to being in major cities or suburbs. So most of the time in low SES neighborhoods, you see a higher rate of depression, bipolar disorders, anxiety disorders, schizophrenia, and severe addictions to drugs and alcohol.
Also, residential segregation is also a huge part of overall well-being as healthy foods are heavily priced and quite scarce, so you would mostly see a majority of fast-food joints in every heavily Black and Hispanic populated neighborhoods, almost in every corner.
It’s almost as if Black and Hispanic neighborhoods are bound to be in situations that are out of their control, and they end up in position of extreme illness.
Yes...it should really say something about the racial disparities both in the system and with how the Doctors’ themselves treat the patients - that black women die at twice the rate as white women from cervical cancer here in the US.
How unnecessary...and preventable.
Part of their business model is fucking over those who have no voice and who society doesn’t pay attention to.
It’s sad and needs to change.
The for-profit days need to end.
JennyDaniella
Stargazer
- MBTI
- INFJ
- Enneagram
- 925
You are right...it is across the whole of healthcare in the US!
Yes...it should really say something about the racial disparities both in the system and with how the Doctors’ themselves treat the patients - that black women die at twice the rate as white women from cervical cancer here in the US.
How unnecessary...and preventable.
Part of their business model is fucking over those who have no voice and who society doesn’t pay attention to.
It’s sad and needs to change.
The for-profit days need to end.
Absolutely agree!!
Skarekrow
~~DEVIL~~
- MBTI
- Ni-INFJ-A
- Enneagram
- Warlock
Another win in the game of bankrupt the ill!!
Had another large sum of medical bills written off!!
Hooray!!!!
This was for a medication issue that sent me to the ER for a couple hours in 2012 (A bill I didn’t even know existed)...and for four booster shots of Cimzia in my stomach at the infusion clinic this last summer that made me sick for over a month.
How much were those three...fairly mundane issues/proceedures they wrote off you might ask?
$15,972.69
Insanity.
This is my share AFTER insurance has paid.
Okay...sure I got enough money in my couch cushions to buy a new fucking car every year.
This is why our medical system is so idiotic.
It’s designed to gouge the sick, ill, elderly, disabled, and poor - to pay the well-to-do shareholders demanding ever higher profits year after year.
I feel very blessed to have had such luck getting these impossible bills out of my life!
Thank you universe (and/or person who approved the write-off)!
:<3white::<3white::<3white::<3white:
Had another large sum of medical bills written off!!
Hooray!!!!
This was for a medication issue that sent me to the ER for a couple hours in 2012 (A bill I didn’t even know existed)...and for four booster shots of Cimzia in my stomach at the infusion clinic this last summer that made me sick for over a month.
How much were those three...fairly mundane issues/proceedures they wrote off you might ask?
$15,972.69
Insanity.
This is my share AFTER insurance has paid.
Okay...sure I got enough money in my couch cushions to buy a new fucking car every year.
This is why our medical system is so idiotic.
It’s designed to gouge the sick, ill, elderly, disabled, and poor - to pay the well-to-do shareholders demanding ever higher profits year after year.
I feel very blessed to have had such luck getting these impossible bills out of my life!
Thank you universe (and/or person who approved the write-off)!
:<3white::<3white::<3white::<3white:
Last edited:
Great news! ♡I feel very blessed to have had such luck getting these impossible bills out of my life!
- MBTI
- infj
- Enneagram
- type 4w5
"healthcare" in this country doesn't really exist. We simply feed the insurance industry with our misery. it's all about making money, and they don't give a crap about you. It doesn't need to be that way, but until congress is no longer owner by their lobbyists nothing will change. and let this sink in. . there is no money to be made in curing you, only in treating you. .
Skarekrow
~~DEVIL~~
- MBTI
- Ni-INFJ-A
- Enneagram
- Warlock
"healthcare" in this country doesn't really exist. We simply feed the insurance industry with our misery. it's all about making money, and they don't give a crap about you. It doesn't need to be that way, but until congress is no longer owner by their lobbyists nothing will change. and let this sink in. . there is no money to be made in curing you, only in treating you. .
Agree 100%
Very sad state.
JennyDaniella
Stargazer
- MBTI
- INFJ
- Enneagram
- 925
I was recently reading into the Utah compromised medical marijuana bill, aka the "Preposition 2 Medical Marijuana Initiative", and I am not happy. Originally, the marijuana laws in Utah was similar to any state that legalized marijuana---however; recently Utah's State Legislature decided to alter the bill and unfortunately make marijuana's accessibility more stricter especially for those that have chronic illnesses and need medical marijuana for other health purposes---those with autoimmune diseases are not qualified for medical marijuana as well. Amount of dispensaries will also be cut down substantially, and access to medical cannabis will have to be through pharmacies. Sound familiar? Sounds like Utah is wanting to make marijuana into the same spectrum of prescription drugs now. Smh.
Church officials from the Church of Jesus Christ of Latter-Day Saints had a huge contribution to this bill's alteration---which made many Utah's citizens infuriated due to the fact that religion and politics should be separated, which I wholeheartedly agree, and many voters are now trying to strike down this new bill.
Healthcare industry is becoming more corrupt over time, and I wonder if things will ever get better at this point. Disappointing.
Church officials from the Church of Jesus Christ of Latter-Day Saints had a huge contribution to this bill's alteration---which made many Utah's citizens infuriated due to the fact that religion and politics should be separated, which I wholeheartedly agree, and many voters are now trying to strike down this new bill.
Healthcare industry is becoming more corrupt over time, and I wonder if things will ever get better at this point. Disappointing.
- MBTI
- INFJ
- Enneagram
- 954 so/sx
Disappointing
And dumb
Zoned Out Again
Newbie
- MBTI
- INFJ
Maternity leave? Ha!!
Nope...nada....some countries even have paid maternity leave...here the woman likely just gets fired for being pregnant and taking time off to give birth.
That sucks!
I guess my country is not as "destroyed" as I thought.
Skarekrow
~~DEVIL~~
- MBTI
- Ni-INFJ-A
- Enneagram
- Warlock
That sucks!
I guess my country is not as "destroyed" as I thought.
Yes...many women here take little more than a week off before going back to work...it’s twisted and it’s sad and it’s going create a whole generation of children who missed bonding with their parent in those first few important months and years.
Then on top of that - many here pay childcare costs that are just as much if not more than their rent or mortgage each month...it’s ridiculously expensive and most of the “affordable” child care places are questionable at best.
If you are lucky enough to have a family member to watch them that is about the best people can do here...they certainly can’t take the time off and expect their job to be waiting for them when they get back.
Many times women will get passed over for a promotion if they make it known that they wish to have children in the near future.
Lame shit.
Skarekrow
~~DEVIL~~
- MBTI
- Ni-INFJ-A
- Enneagram
- Warlock
I was recently reading into the Utah compromised medical marijuana bill, aka the "Preposition 2 Medical Marijuana Initiative", and I am not happy. Originally, the marijuana laws in Utah was similar to any state that legalized marijuana---however; recently Utah's State Legislature decided to alter the bill and unfortunately make marijuana's accessibility more stricter especially for those that have chronic illnesses and need medical marijuana for other health purposes---those with autoimmune diseases are not qualified for medical marijuana as well. Amount of dispensaries will also be cut down substantially, and access to medical cannabis will have to be through pharmacies. Sound familiar? Sounds like Utah is wanting to make marijuana into the same spectrum of prescription drugs now. Smh.
Church officials from the Church of Jesus Christ of Latter-Day Saints had a huge contribution to this bill's alteration---which made many Utah's citizens infuriated due to the fact that religion and politics should be separated, which I wholeheartedly agree, and many voters are now trying to strike down this new bill.
Healthcare industry is becoming more corrupt over time, and I wonder if things will ever get better at this point. Disappointing.
This is all the doing of the Mormons and their backward BS.
(I can say that, I was raised one)
Make it into a pill and call it something else and market it and they will take it as medicine without a second thought...but they are too fucking stupid to see the difference and so those who really need the extra help with pain or anxiety have to work extra hard on top of already working extra hard just to get access to something proven to be safer than alcohol (which the Mormons don’t drink) and certainly safer than opioids which everyone is nutting up over unnecessarily.
Again...those people who abuse their prescriptions...or with callous doctors who do not understand you cannot just stop someone who has been taking them long term and NOT fuck them up...those who order non-prescribed medication from China with norfentanyl in it are ODing like Prince.
So it must be the medication and not how it is being used and prescribed (sarcasm), and THEN tapered off with all the support medication made available to someone needing it...then follow ups are needed and possibly counseling as people can have issues feeling happy without medication.
So yeah...that is a problem.
But don’t make it more difficult for someone like me with a legit issue of Ankylosing Spondylitis, known to be quite up there on the pain scale -
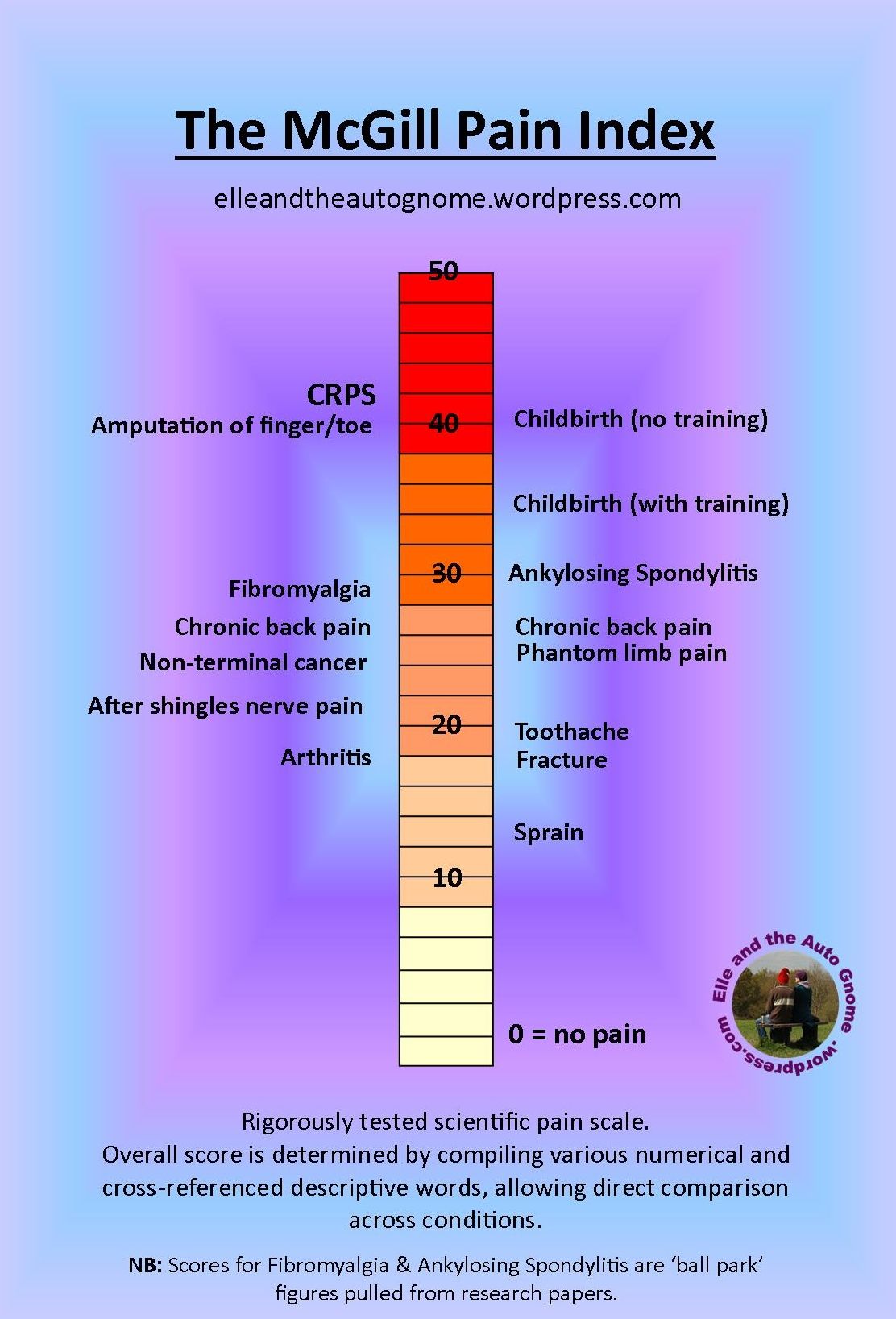
(Ball park...isn’t it all subjective to the person anyhow?)
There is ONE pain clinic that still has maintained prescribing opioids close by me...all the rest have been scared off...the primary care doctors who should be treating pain are not, because once again, they are too scared AND basically don’t have time to fill out all the extra pages of paperwork required to be submitted for such prescriptions.
I have actually substantially lowered my dose of medication over the years and am now on very low amounts, especially considering what I once was on at one point in time.
And yet...if my insurance changes or some shit like that...I could easily have a very difficult time maintaining the medications that I have maintained if not lowered for years and years with no issues of addiction that have plagued me.
It really irritates me that I now have to drive to the office to pick up a paper prescription...I understand they are trying to cut down on fake prescriptions but you are really inconveniencing people who already have a difficult time physically functioning.
It’s like the ATM card issued to me by SS disability...it doesn’t work at the gas pump...you have to go in and use it at the register - again, it’s very small shit...and the normal person wouldn’t notice or care...but some days it makes a hell of a difference walking that 20ft.
lol
Ranting now...
My pain clinic is rad...they are totally cool with marijuana use, so long as it doesn’t become a problem or cause issues with your own meds.
Keeping my fingers crossed that I can go to them for a long while.
It’s nearly impossible to find a pain doc that doesn’t want to drop all your pain meds and put you on gabapentin and physical therapy.
Motherfuckers.
Severe case of apathy and inability to empathize with those suffering.
Been there...done that....it is cruel and it doesn’t address my pain other than making it worse to the point I am non-functional and I cannot afford to go to physical therapy 3 times a week thank you very fucking much - that would be $60 a week so $240 a month?
Simply not affordable and not helpful.
I have found many “pain” doctors to be incredibly callous and quick to place blame on you rather than the illness.
There is a pretty lengthy and nasty Web MD review out there I wrote about a particular gal I saw.
Such a horrible person...uncaring...apathetic...suspicious...treated everyone like drug seekers regardless of their actual reason for being in pain.
Like everyone ended up there for made up reasons...fucking twat.
Last edited:
just me
Well-known member
- MBTI
- infj
It makes one wonder: does the government that implemented affordable health care own the insurance companies? If a person lives alone and makes $30,000 a year, they get zero credit to an almost impossible already insurance rate with poor coverage. They are talking about $2000 base rate insurance coming....a month. Doing the math, they punish a person for not having insurance. Who can afford $24,000 a year health insurance rates? That would leave $500 a month left. Now, if you lie about your income, it's alright for some people to make their numbers look right. If you make minimum wage, your cost will be alright. If your spouse is over 65, they count their income with yours.
Now, they are closing down those doctors that don't show due diligence with their prescriptions for their patients. Nothing wrong with that. Then, they get all the pharmacies to use the same generic med that does not offer any relief from pain and still call it a narcotic. After taking those a month, a person hurts all over. Why? Meds we can't afford without insurance are becoming somewhat useless.
Makes a person want a joint? Won't stop chronic pain.
Now, they are closing down those doctors that don't show due diligence with their prescriptions for their patients. Nothing wrong with that. Then, they get all the pharmacies to use the same generic med that does not offer any relief from pain and still call it a narcotic. After taking those a month, a person hurts all over. Why? Meds we can't afford without insurance are becoming somewhat useless.
Makes a person want a joint? Won't stop chronic pain.